The Dopaminergic System refers to three neurotransmitters, Dopamine, Noradrenaline and Adrenaline.
The Dopaminergic Chain refers to how we create (synthesise) neuronal Dopamine first, unused Dopamine is then converted to Noradrenaline, unused Noradrenaline is then converted to Adrenaline. Unused Adrenaline is then turned into easy to excrete products (eg urine).
If you struggle to make enough Dopamine, you will struggle to make enough Noradrenaline. This is common in ADHD. Another form of ADHD shows another potential problem people can have with the Dopaminergic System, where too much Dopamine is converted to Noradrenaline, undermining your ability to use the Dopamine for things like higher order thinking (executive function).
If you struggle to make enough Dopamine, you will struggle to make enough Noradrenaline. This is common in ADHD. Another form of ADHD shows another potential problem people can have with the Dopaminergic System, where too much Dopamine is converted to Noradrenaline, undermining your ability to use the Dopamine for things like higher order thinking (executive function).
You may also be interested in
International Compatibility
The USA and Canada have a different naming convention.
- Adrenaline = Epinephrine.
- Noradrenaline = Norepinephrine.
Understanding the Dopaminergic System
Synthesis / Production
As stated above, for neuronal Dopamine, Noradrenaline and Adrenaline, we cannot use the chemicals created by the adrenal glands. That means that our brains need to make it locally. The Dopaminergic Chain refers to how Dopamine is made first. Some Dopamine is converted to Noradrenaline. Some Noradrenaline is converted to Adrenaline. Each of these are stored in reservoirs, mostly at the end of the axons, the branches that lead away from neurons, at the synaptic gap in vesicles.
Production Sites and Pathways
Dopamine is made in two different regions. The majority is made in the adrenal glands just above your kidneys, however that does not get used by your brain. The Blood Brain Barrier stops your adrenally produced Dopamine from being available to your brain, so we humans evolved to make a second batch of Dopamine in our mid-brains, in the Ventral region.
Dopaminergic Production Sites
Dopamine is produced in the middle brain, at glands called:
- Substantia Nigra
- Ventral Tegmental Area (VTA)
- Hypothalamus
- Dorsal Striatum
- Substantia Nigra Pars Compacta (SNc)
Noradrenaline and Adrenaline are produced from the Dopamine.
Dopaminergic Production
Dopamine is made by metabolising certain foods. If you have an insufficiency of any of these, it will interfere with healthy production of Dopamine.
- Tyrosine.
- Vitamin B6.
- Vitamin C.
- Iron / Ferritin.
See Dietary Vitamins and Minerals for information about these.
- Dopamine is made first.
- Tyrosine is extracted from relevant protein (mostly animal meat or soy beans) via digestion, which is then converted to L-Dopa (Levodopa) using B6, C and Iron. L-Dopa is added to your blood to be transported around your body.
- L-Dopa passes the Blood Brain Barrier (BBB).
- The Dopamine made in your adrenal gland can’t get to your brain as it can’t pass through the BBB.
- This is why you don’t treat ADHD by ingesting or injecting Dopamine. Instead, medication like amphetamines prompt your brain to make more than it was going to.
- L-Dopa is converted into Dopamine in the middle brain, at glands called Substantia Nigra, Ventral Tegmental Area (VTA), Hypothalamus, Dorsal Striatum and Substantia Nigra Pars Compacta (SNc).
- Dopamine is distributed to parts of your brain as described above in Dopamine Pathways.
- Noradrenaline is made from Dopamine via Vitamin C. [Source]
- Noradrenaline is converted to Adrenaline by attaching a methyl group.
- Methyl groups are relatively common, so no specific dietary intake is required for this once you have produced Noradrenaline.
Dopamine
Dopamine is a complex hormone that has a number of functions throughout the body that regulate the metabolic system. Within the Blood Brain Barrier, Dopamine is used as a neurotransmitter, passing certain types of signals at the synaptic gap from one neuron to another neuron. Different areas of the brain use Dopamine to regulate different kinds of brain activity, for example, the Medial Prefrontal Cortex (mPFC) appears to contain a collection of systems that we call the Executive Function.
Neurologically speaking, Dopamine in our PFC (prefrontal cortex) helps us to be creative, connect ideas to other ideas and understand the deeper layers of nuance – the Executive Function. Too much and our creativity can decrease and we risk psychosis, too little and our understanding of nuance and depth drops. In our cerebellum Dopamine is used to control our muscles, creating smooth and accurate movements. Low Dopamine here can cause a spectrum of problems, from clumsiness, dyspraxia, restless leg syndrome and Parkinson’s Disease.
We manufacture only so much Dopamine a day. For most people (neurotypicals), this can rise and fall a bit depending on our needs. If we think too hard, or do too much physical activity, we deplete our reserves and can run low. This will prompt us to want to do less so that we can recover our stores by generating more.
Neurological Dopamine Systems
Dopamine specifically acts as a neurological transmitter, aka neurotransmitter. Neurotransmitters are one of a number of different chemicals that our brain uses to fill the synapse gap between different neurons. We have covered this in detail in the Neurotransmitters page.
Our brain has a number of different Dopamine Systems, where the Dopamine acts to enable certain different abilities throughout this system, mostly described as parts of the Executive Function (EF), and any skill that you learn. A modulation (decrease or increase) in Dopamine will affect how effective the network of neurons in these regions work. Most are beyond the scope of this page.
Dopamine has a profound effect on our EF. We use the EF to be present, make choices, understand things, and solve problems. Insufficient Dopamine or problems with Dopamine receptors can lead to Executive Dysfunction.
Dopamine Distribution Pathways
Dopamine is distributed from synthesis sites to our brain via pathways:
- Mesocorticolimbic system
- Dopamine Source: is produced in the VAT (Ventral Tegmental Area) and distributed to the cortical and limbic areas.
- Mesolimbic pathway
- From the VAT, Dopamine is carried first to the frontal lobes (the front 1/3 of your brain), then up to the top of your brain, then back to the top back of your head, above the cerebellum.
- Mesocortical pathway
- Crom the VAT, Dopamine is carried to the Prefrontal Cortex (PfC), the brain just behind your forehead bone.
- Nigrostriatal pathway
- Dopamine Source: is produced in the Dorsal Striatum and Substantia Nigra Pars Compacta (SNc).
- The Dopamine pathway moves mostly upwards and a little forwards to provide Dopamine to your middle brain region, mostly the dorsal area.
- More, Nigrostriatal pathway Wikipedia
- Tuberoinfundibular pathway
- Dopamine Source: is produced in the Hypothalamus.
- The Dopamine pathway moves to the pituitary gland.
- More, Tuberoinfundibular pathway Wikipedia
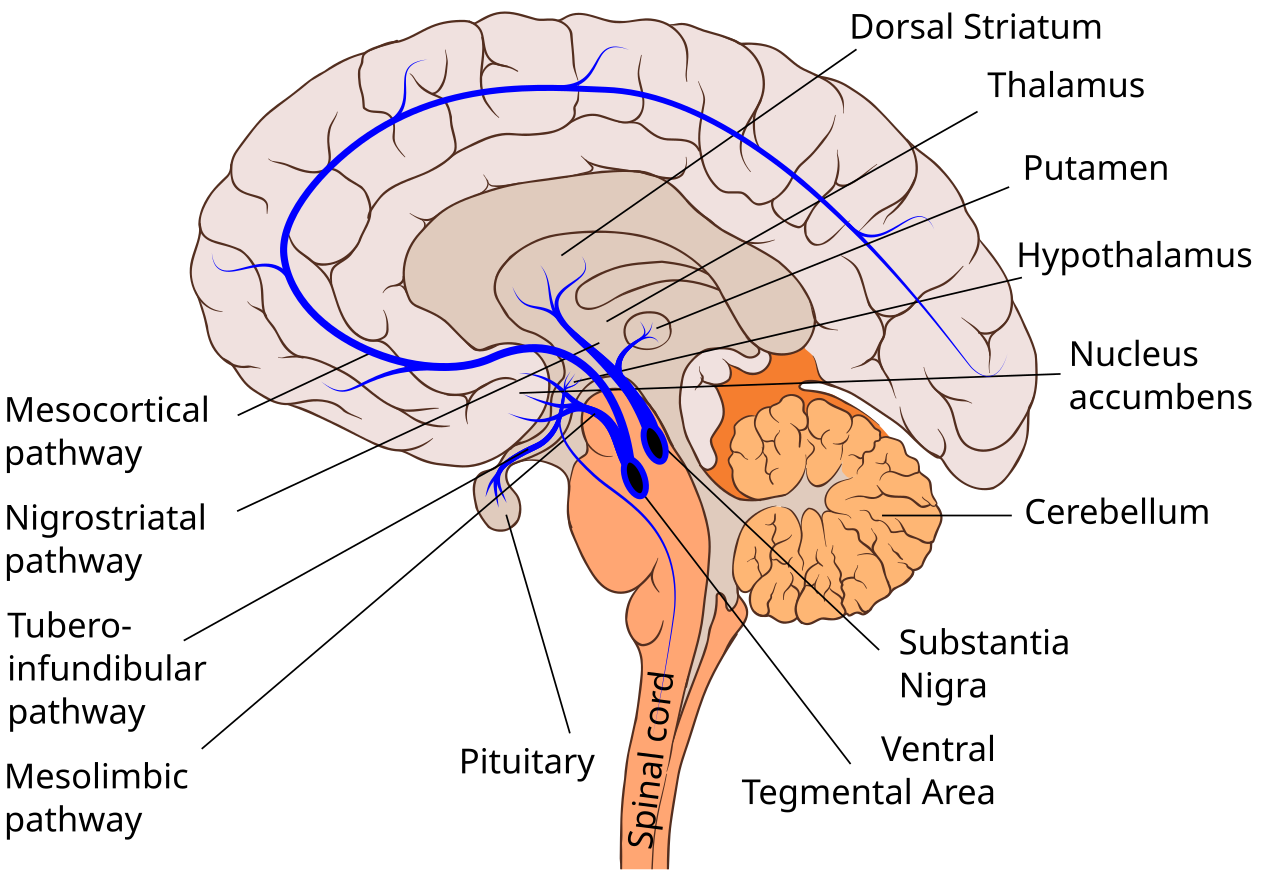
Slashme; Patrick J. Lynch; User:Fvasconcellos, CC BY-SA 4.0, via Wikimedia Commons
Your brain tries to keep the production of Dopamine, Noradrenaline and Adrenaline homeostatically relevant, making more when you need it, and less when you don’t. A way to think of this is the concept of the Goldilocks Zone – if you are too low, it makes more, if you are too high it slows production, stops production, or converts the excess to something else.
Dopamine Reward System
The Dopamine Rewards System releases a small amount of Dopamine to the PFC are anything that our ancient ancestors would have found beneficial. Our biology tries to reward us for doing things that improve our survival.
Dopamine Chasing Foods aka The Dopamine Diet
When we were hunter gatherers, types of food that were hard and highly rewarding were things that can be broken down to glucose, various amines and salt. Salt was easy to get at the coast of the oceans, or in the middle of deserts, but hard to get everywhere else. Each of these has an important role to play in how we think and feel.
Brief Version
The core Dopamine Chasing Foods are:
- Fat
- Carbohydrates
- Sugars
- Protein
- Salt
None of these foods are inherently bad, when part of a balanced diet. Often, when diets are out of balance such as eating disorders, these foods become the primary ratio of food, and the foods that should be the in majority are too low. For more information on what a well balanced healthy diet looks like, check out Nutrition, Health in Body and Mind.
When we eat these foods, our brain releases some stored Dopamine and Endorphins Neurotransmitter to reinforce the behaviour (eating those foods). With the increase in glucose (from the food), Dopamine and Endorphins, we can think more clearly, push ourselves harder and stabilise our mood. This can benefit in thinking and feeling can lead to a complex reinforcing feedback loop that is at the core of many eating disorders.
Details
Making Dopamine was covered above in the the Dopaminergic Synthesis. It relies on B6 to help extract the amino acid Tyrosine from the consumed protein. We use B6, Vitamin C (Ascorbic Acid) and Ferritin to convert Tyrosine into L-Dopa and then finally into Dopamine. Oestradiol is used at the gland that produces Dopamine in the brain to regulate the rate of Dopamine production, so if your Oestradiol is low, you will have low production of Dopamine.
Looking at the Dopamine Chasing Foods:
- Fat:
- When we crave fatty food, we generally crave trans and saturated fats. When we ingest this, we extract long chain cholesterol. LDL Cholesterol is a key ingredient that we generate primary sex hormones with, which we use to make Oestradiol.
- The creamy texture from fatty foods often create a “nice mouth feel”, which stimulates the release of endorphins. Endorphins help us feel less pain and more joy, increasing the efficiency of releasing and producing Dopamine. Effectively, this helps boost how much Dopamine we generate and release.
- Carbohydrates (simple and complex sugars):
- Our brains are very expensive organs to run. Our brain consumes 20% of our bodies resources. When we think hard, our frontal cortex can deplete our blood sugar quite rapidly in the absence of physical exertion, and on low blood sugar our brain can reduce thinking. This exacerbates the brain fog of low Dopamine in our frontal cortex. Adding glucose to our system in the form of sugars (lactose, fructose and sucrose) and carbohydrates that we can break down into glucose, will trigger a release of sugar into our blood, tricking our frontal cortex to operate again.
- We often get a small endorphin surge when we eat sweet foods, which improves Dopamine production and release.
- Protein
- Tyrosine is the base building block for Dopamine, which is the precursor for Noradrenaline to maintain our amygdala (mood, sense of safety), which is a precursor for Adrenaline which we use to increase our alertness and mental arousal.
- The amino acid Tyrosine can be extracted from animal meats, Phenylalanine and some artificial sweeteners.
- Animal meat comes with its own B6, which is an important catalyst for extraction and conversion of Tyrosine into Dopamine.
- Unfortunately, most of the protein we crave in the junk food category are low in Tyrosine and B6.
- Salt:
- For our frontal cortex to operate, neurons need to communicate with each other. A neuron sends a signal down the Axon towards the Synaptic Gap, where we use Dopamine as the neurotransmitter to act as an on switch for the signal. The Axon works by cascading sodium and calcium ions – sodium (Na+), potassium (K+), chloride (Cl−), and calcium (Ca2+).
- Common table salt contains both sodium and chloride, two of the primary ingredients we need for this signal.
- Our body can leach calcium from our bones if necessary, but we may crave dairy for both fat and calcium.
- Some complex salts in junk food include potassium.
- Common signs of Potassium deficiency
- weakness and fatigue
- feeling tired
- muscle cramps
- an abnormal heart rhythm (arrhythmia -skipped heartbeats or an irregular heartbeat)
- Common signs of Potassium deficiency
- For our frontal cortex to operate, neurons need to communicate with each other. A neuron sends a signal down the Axon towards the Synaptic Gap, where we use Dopamine as the neurotransmitter to act as an on switch for the signal. The Axon works by cascading sodium and calcium ions – sodium (Na+), potassium (K+), chloride (Cl−), and calcium (Ca2+).
Effectively, the foods that we eat when we are feeling dysregulated in mood and thinking contain the most common base ingredients that we would be deficient in if we are struggling to think: sugars, salts and Dopamine ingredients.
While the can be bottlenecks for creating Dopamine, these are not the cause of ADHD. Insufficiency in these ingredients in your diet will merely exacerbate ADHD. These insufficiencies can be quite common. Unfortunately, your brain doesn’t factor in that you didn’t take your medication, or that your medication is insufficient, and prompts you to go and eat foods that contain the above instead of reminding you to take your meds.
Reward and Reinforcement
Dopamine if often sited as the Reward and Reinforcement Chemical. This is partially true, but often grossly misrepresented.
Dopamine is used to process information and solve problems. At a neuronal level, when we get something right, we want that correct way to be reinforced. Dopamine and Endorphins are used to reinforce that pathway. When we get something wrong, we don’t want to encourage that pathway, so Dopamine is decreased, making it harder for that path to work.
Imagine an overgrown garden. Paths that are useful have people and animals walking on them, so the path seems fairly clear. Paths that are inefficient are often skipped, so they become overgrown, which further makes then less likely to be used. That’s effectively what the Dopamine is doing, making efficient pathways better and neglecting the inefficient pathways which leads to them returning to a wild state.
A theory around Dopamine Addiction through poor reward methods exists, but in my opinion this is either rare or misunderstood. See below, Dopamine Addiction.
Dopamine Addiction
It is possible to acquire a Dopamine addiction by over using strong amphetamines (above ADHD dose). While this is thought to be common, it is probably very rare. Mostly what people are thinking of when they think about Dopamine based addictions is Self-Medication for undiagnosed and unmedicated conditions, most of which are congenital. When those conditions are properly diagnosed and medicated, most people’s addictions dissipate.
The theory about Rewards leading to Dopamine Addiction were formed before ADHD was properly understood. Most neurotypical brains have easy access to Dopamine, so while the Dopamine Reward for success is nice, it isn’t that nice that addictive level behaviours are formed. For someone who has a Dopamine insufficiency, such as ADHD, that Dopamine Reward feels really good. Not only does the Endorphins release feel nice, but the ability to think clearly and feel your mood regulate is a state of existence that you will want to return to.
The problem wasn’t the Rewards leading to Dopamine Addiction. The problem was the insufficiency of Dopamine. Because the early psychologists and psychiatrists did not understand how Dopamine worked (very modern medicine), they were left to try to explain why some experiences led to addiction behaviour in the absence of knowing that many people have undiagnosed ADHD.
We cover this quite extensively in our Understanding Addiction page.
Dopamine Receptors
There are five types of dopamine receptors, which include D1, D2, D3, D4, and D5. Each receptor has a different function and is found in different locations.
The function of each dopamine receptor[4]:
- D1: memory, attention, impulse control, regulation of renal function, locomotion
- D2: locomotion, attention, sleep, memory, learning
- D3: cognition, impulse control, attention, sleep
- D4: cognition, memory, fear, impulse control, attention, sleep
- D5: decision making, cognition, attention, renin secretion
The five different dopamine receptors can subdivide into two categories. D1 and D5 receptors group together (Dop Alpha for here), and D2, D3, and D4 are together in a separate subgrouping (Dop Beta).
{D1 to D5 receptors, source: Biochemistry, Dopamine Receptors}
Noradrenaline
Noradrenaline is a neurotransmitter and hormone that has many uses. The most important in Mental Health is how it affects our Amygdala, which affects our mood regulation.
Mood: Threat Detection and Priorities
The Amygdala is a part of your brain that’s major purpose is running Brain Mode 1 – Questions & Answer Sets and our Threat Detection as part of our Fear Reflex. The Amygdala is the seat of our cognitive function before we go through puberty. While it is possible for pre-pubescent people to have a level of deep understanding about things, their depth is quite shallow compared to the adult level that is possible after puberty evolves the prefrontal cortex and the brains higher order thinking shifts to be Dopamine dominant.
The Amygdala is closely tied in with your cerebellum, which processes your sensory inputs. You sense things via your eyes, ears, nose, mouth, touch and so on. This is piped to your cerebellum (hindbrain just above your spine). A sneak peak is sent to your Amygdala to compare to your thalamus and hypothalamus (raw memory) and if it matches “problem”, your Amygdala communicates this recognition or a problem to your conscious brain (mostly the frontal lobes) as one of 3 primary “not safe” feelings – fear (pain is expected), anger (a problem needs solving) or disgust (this will sicken you). If it can’t determine which of those 3 categories fit, you will feel a sense of “general unease”, aka dysphoria. If your Amygdala does not match your raw sensory data to a pattern of threat, it gives you the feeling of ease, or “safe”.
The sensory data is then further developed and made into the 3 dimensional sensory map that you think you are perceiving by your cerebellum using various other parts of your brain to turn the raw sensory data into something useful.
If you feel “safe”, your priorities are resting, healing, mending, creative preparation and socialising. If you feel “not safe”, then your priority is to cognitive identify the source of the problem and fix it. The lower the urgency, the more creative our solutions, the higher the urgency, the more primal our solutions (Freeze, Fawn, Flight, Fight).
Your Amygdala mostly uses Noradrenaline as the key neurotransmitter to do this threat detection, much like your frontal lobes mostly use Dopamine. If your Amygdala can’t get enough Noradrenaline, or it gets too much Noradrenaline, your Amygdala cannot correctly identify “safe” or “not safe”, so you get the feeling of “general unease”. We feel dysphoric. Our frontal lobes receive this feeling, and from this message, it will try to identify the external cause of the unease. Unfortunately, beyond a coincidental problem, it can’t because the problem is your Noradrenaline is outside of the Goldilocks Zone.
If this were a short term problem, we’d be on a higher level of alert for a few minutes or hours, then shrug it off as a weird experience.
Often, this is a long term, lifelong problem. The “general unease” just doesn’t go away, unless we indulge in substances, risky behaviour (to find something to blame for the cause), or take medication. Ongoing “general unease” is interpreted by our brains as either Anxiety or Aggression / Anger.
If we normally have sufficient Noradrenaline for our Amygdala to correctly report the threat level of the current circumstances, but we then run out of Dopamine, our brain will switch to Critical or Crisis Mode, which can change the effectiveness of our Amygdala.
Biological Conditions and Feedback
A few non-brain conditions can affect the level of neuronal Noradrenaline and Adrenaline, such as cardiopulmonary conditions, and chronic fatigue syndrome.
Our neuronal Noradrenaline and Adrenaline attempt to match the levels that are represented in our bodies, and if those are out, we can feel their effect on our mood. This is also true in reverse, if you detect a threat, the elevation in your neuronal Noradrenaline and Adrenaline will then be reflected in your body as you ramp up to meet the Fight / Flight outcome.
Adrenaline
Adrenaline (Epinephrine in the USA) plus moderate blood sugar is needed to store long term memories. If your Adrenaline is high, you’ll be triggered into Crisis Mode, and if it is low you’ll be pushed into Depression. Both of these take away from your ability to think clearly and make wise decisions.
Common Neurological Dopaminergic Conditions
ADHD
Neurotransmitter Cause: Low Dopamine at dendritic dopamine receptors in the PFC
ADHD is a congenital, highly heritable neurological condition where the receiving dopamine receptors in the prefrontal cortex (PFC) do not get enough activation by Dopamine. This can be due to either the ADHDer not making enough Dopamine, and or not retain sufficient Dopamine, and or the Dopamine is too quickly converted to Noradrenaline. Insufficient Dopamine receptor activation in the PFC leads to poor Executive Function, that is, difficulties in:
- Decision making
- Impulse control
- Being present (disassociation)
- Remembering long term information
- Retaining short term information
- Staying on track
and so on.
ADHD Medication can often help with Dopamine creation, retention, synaptic delivery and efficiency in our PFC depending on which version of ADHD you may have.
More: ADHD, ADHD Neurology.
Anxiety
Neurotransmitter Cause: Mostly low Noradrenaline, sometimes high Noradrenaline or body adrenals.
Anxiety is a natural human feeling to prepare us for a potential problem. Anxiety is the feeling you get when you are prepared for action, but don’t know what that action is – this is natural and not a problem when it is occasional.
If Anxiety becomes a common feeling then something is wrong and you may have an Anxiety Disorder.
Anxiety disorders are most commonly a biological cause, generally neurological and sometimes related to other biological systems such as cardiopulmonary (heart and lungs) or hormones. In rare circumstances, Anxiety may be related to a traumatic experience which has led to maladaptive over-preparedness.
The most common causes is either Noradrenaline outside of the Goldilocks Zone (too low {most}, too high {rare}), or the body’s adrenal system as part of the cardiopulmonary system. See ‘Mood: Threat Detection and Priorities‘ above in the Noradrenaline section to understand how this works.
If your Noradrenaline is low, you’ll likely find that caffeine is calming. Likely you’ll find benefit with an NRI.
If you avoid caffeine, especially if you find that you are agitated on a single regular serving (between 40 to 90 mg), then you probably either have high neuronal Noradrenaline, or your bodies Adrenal system is over the top. Likely you’ll benefit from Clonidine or a Beta Blocker (so long as your blood pressure is average to high).
More: Anxiety, Anxiety Neurology
Depression
Neurotransmitter Cause: Low Noradrenaline + low Adrenaline.
Schizophrenia
Neurotransmitter Cause: Approximately half caused by excess triggering of D2 Dopamine receptor; possibly 40% high Noradrenaline induced psychosis, which may be triggered by high oestradiol.
Around half of people diagnosed with Schizophrenia are sensitive to having excess Dopamine over activating the D2 Dopamine Receptor. This over triggered Dopamine receptors triggers other neural network pathways that interfere with reality checking. This can usefully increase to creativity as various creative ideas that may be useful are not discarded too quickly. The challenge is to be able to tell the difference, and with the inhibition of the Reality Checker brain module, this is very hard to do. The combination is confusion, where the Schizophrenic Person can’t confidently tell what is real and what is not.
There is some fascinating research that shows that a commonality in psychosis is a the D2 receptor triggering a pathway to the Serotonin 5-HT2A receptor. Blocking only the D2 receptor and blocking only the 5-HT2A receptor doesn’t seem to strongly affect psychosis, so currently the hypothesis is the intermediary glial cell may be the core part of the disorder. More research is needed.
Schizophrenia can be misdiagnosed when the condition is more caused by an excess Noradrenaline in the midbrain, often managed well with Noradrenaline reducing or moderating medications such as Clonidine.
Voice Hearing is not Schizophrenia, although there is a common co-occurrence (many Schizophrenic People ‘hear’ voices).
Movement Disorders
The Cerebellum (just above your spine) is the part of your brain that smooths physical and cognitive movements. The Cerebellum uses Dopamine to regulate your movement.
If you have the ADHD version where you struggle to make enough Dopamine for your PFC, then you probable also struggle to make enough for the rest of your brain. This can lead to various diagnoses of movement disorder.
Dyspraxia / Developmental Coordination Disorder
Neurotransmitter Cause: Mostly low Dopamine
DCD is considered to be a lifelong neurodevelopmental condition that significantly impacts a person’s ability to plan and execute coordinated motor skills. DCD has a prevalence of 5-6% (5 to 6 out of 100 people) [“DCD Overview”, DCD Australia], unless you look at the population of ADHDers, where it is as high as 81.5%, where children who were taking ADHD medication received significantly lower DCD-Q scores (improved DCD) [“Motor skills in children with ADHD: overlap with developmental coordination disorder”, Springer Nature].
What this tells us is that DCD is not just a developmental disorder, as named, but is primarily a problem with Dopamine delivery to the Cerebellum.
Parkinson’s Disease
Neurotransmitter Cause: Mostly low Dopamine and Dopamine production issues
Parkinson’s disease is a progressive neurodegenerative disorder, mainly in the central nervous system. It affects both motor and non-motor systems, however it is most famous for how the effect on motor systems affects movement causing symptoms like tremors, jerky movements, stiffness, and slow movements.
Pathophysiology involves progressive degeneration of nerve cells in the Substantia Nigra, a midbrain region that synthesises (produces) Dopamine and provides it to the Basal Ganglia (mid-brain) near to the Substantia Nigra. This part of your brain is involved in voluntary motor control. Without enough Dopamine, your brain struggles to manage smooth and accurate movements, leading to either erratic twitches, over movement (reaching too far), freezing, or slow movements.
Non-motor symptoms develop later in the disease and include behavioural changes and or neuropsychiatric problems such as sleep abnormalities (too much, too little, interrupted), psychosis (altered perceptions), and mood swings.
The aetiology (cause) for Parkinson’s Disease is not known.
More: Wikipedia has an excellent page on Parkinson’s Disease.
Restless Leg Syndrome
Neurotransmitter Cause: If not low ferritin, mostly low Dopamine
RLS is a movement disorder where you feel like you have to move, and this movement ends up in a repetitive loop. It can occur to arms and legs, despite the name. The prevalence of RLS is around 1 in 10 people, with clinical levels around 2-3% (2 or 3 people out of 100) [“Restless legs syndrome”, Mayo Clinic]. The prevalence in a group of ADHDers was 34.5%, and a systematic review showed reports from as little as 11% to as high as 54% [
The most effective treatment is iron, if your ferritin serum is low. If that doesn’t work, the next best medication is Dopaminergic Agents [“Treatment of restless legs syndrome: An evidence-based review and implications for clinical practice”, Trenkawlder et al]. There are some other medications that can be effective, read the article to find out.
What this tells us is that medications that can change (increase) the expression or management of Dopamine, Noradrenaline and Adrenaline affect RLS, when iron deficiency is not the key factor.
Tic Disorders & Tourette’s Syndrome
Neurotransmitter Cause: Mostly low Dopamine and high adrenals.
Tics are sudden, repetitive, involuntary movements or sounds. A specific tic disorder is called Tourette’s Syndrome. [“Tics and Tic Disorders”, Cleveland Clinic]
Tics are considered to be from a form of neurodevelopmental occurrence, typically starting in childhood (around 5 years old).
While tics can be suppressed for short periods, doing so usually causes significant tension, making the tic eventually unavoidable. That is, you feel that you need to move suddenly, and if you can suppress it, the need to move escalates until you can’t hold back.
As an experiment, try holding your breath for twice as long as you think you can. It won’t harm you to do so (under 3 minutes is very safe). At around the time you usually stop holding your breath, you may be able to choose to hold it for a bit longer. Before you reach the double point, you’ll probably find that you’ve given up and breathed.
Why?
Some part of your brain has decided that your cognitive decision to suppress the action (breathing / tic) is wrong and overrides you.
Compared with children not diagnosed with ADHD, children with ADHD were 4.1 (7 year old) to 5.9 (10 year old) times more likely to have Chronic Tic Disorder [“Chronic tic disorders in children with ADHD”, William et al]. According to the “Canadian Guidelines for Evidence”Canadian Guidelines for the Evidence-Based Treatment of Tic Disorders: Pharmacotherapy“, the best two medications for Chronic Tic Disorder (regardless of ADHD), are Clonidine and Guanfacine. Both of these medications help improve Dopamine and mitigate Noradrenaline and Adrenaline. Medications that were given a weak recommendations were antipsychotics, botox and cannabinoids.
What this tells us is that most Chronic Tic Disorders are related to the Dopaminergic system, likely low Dopamine and high Noradrenaline.
Further Resources:
- Role of Serotonin in Central Dopamine Dysfunction
- Medial prefrontal cortex in neurological diseases
- Binding of antidepressants to human brain receptors: focus on newer generation compounds
- Comparative pharmacology of selective serotonin re-uptake inhibitors (SSRIs)
- Sequential improvement of anxiety, depression and anhedonia with sertraline treatment in patients with major depression
- The Role of D2-Autoreceptors in Regulating Dopamine Neuron Activity and Transmission
References
Source Bhatia, A., & Saadabadi, A. (2023, June 22). Biochemistry, Dopamine Receptors. PubMed; StatPearls Publishing. https://www.ncbi.nlm.nih.gov/books/NBK538242/
Di Giovanni, G., Esposito, E., & Di Matteo, V. (2010). Role of Serotonin in Central Dopamine Dysfunction. CNS Neuroscience & Therapeutics, 16(3), 179–194. https://onlinelibrary.wiley.com/doi/abs/10.1111/j.1365-2710.2000.00302.x
Xu, P., Chen, A., Li, Y., Xing, X., & Lu, H. (2019). Medial prefrontal cortex in neurological diseases. Physiological Genomics, 51(9), 432–442. https://doi.org/10.1152/physiolgenomics.00006.2019
Cusack, B., Nelson, A., & Richelson, E. (1994). Binding of antidepressants to human brain receptors: focus on newer generation compounds. Psychopharmacology, 114(4), 559–565. https://doi.org/10.1007/bf02244985
Hyttel, J. (1993). Comparative pharmacology of selective serotonin re-uptake inhibitors (SSRIs). Nordic Journal of Psychiatry, 47(sup30), 5–12. https://doi.org/10.3109/08039489309104119
Boyer, P., Tassin, J. P., Falissart, B., & Troy, S. (2000). Sequential improvement of anxiety, depression and anhedonia with sertraline treatment in patients with major depression. Journal of Clinical Pharmacy and Therapeutics, 25(5), 363–371. https://doi.org/10.1046/j.1365-2710.2000.00302.x
Ford, C. P. (2014). The Role of D2-Autoreceptors in Regulating Dopamine Neuron Activity and Transmission. Neuroscience, 282, 13–22. https://doi.org/10.1016/j.neuroscience.2014.01.025
Bhatia, A., Lenchner, J. R., & Saadabadi, A. (2023). Biochemistry, Dopamine Receptors. PubMed; StatPearls Publishing. https://www.ncbi.nlm.nih.gov/books/NBK538242/#
Nigrostriatal pathway. (2023, December 31). Wikipedia. https://en.wikipedia.org/wiki/Nigrostriatal_pathway
Forero-Girón, A. C., & Toro-Labbé, A. (2025). How does dopamine convert into norepinephrine? Insights on the key step of the reaction. Journal of Molecular Modeling, 31(1). https://doi.org/10.1007/s00894-024-06256-w
Tuberoinfundibular pathway. (2022, October 21). Wikipedia. https://en.wikipedia.org/wiki/Tuberoinfundibular_pathway
Cleveland Clinic. (2022, March 27). Norepinephrine: What it is, function, deficiency & side effects. Cleveland Clinic. https://my.clevelandclinic.org/health/articles/22610-norepinephrine-noradrenaline
DCD Overview. (n.d.). DCD Australia. https://dcdaustralia.org.au/what-is-dcd-2/
Meachon, E. J., Schaider, J. P., & Alpers, G. W. (2025). Motor skills in children with ADHD: overlap with developmental coordination disorder. BMC Psychology, 13(1). https://doi.org/10.1186/s40359-024-02282-8
Trenkwalder, C., Hening, W. A., Montagna, P., Oertel, W. H., Allen, R. P., Walters, A. S., Costa, J., Stiasny-Kolster, K., & Sampaio, C. (2008). Treatment of restless legs syndrome: An evidence-based review and implications for clinical practice. Movement Disorders, 23(16), 2267–2302. https://doi.org/10.1002/mds.22254
Mayo Clinic. (2018). Restless legs syndrome – Symptoms and causes. Mayo Clinic. https://www.mayoclinic.org/diseases-conditions/restless-legs-syndrome/symptoms-causes/syc-20377168
Poh, W., Payne, J. M., Gulenc, A., & Efron, D. (2018). Chronic tic disorders in children with ADHD. Archives of Disease in Childhood, 103(9), 847–852. https://doi.org/10.1136/archdischild-2017-314139
Cleveland Clinic. (2024, August 19). Tics and Tic Disorders: What They Are, Causes & Types. Cleveland Clinic. https://my.clevelandclinic.org/health/diseases/tics-and-tic-disorders
Pringsheim, T., Doja, A., Gorman, D., McKinlay, D., Day, L., Billinghurst, L., Carroll, A., Dion, Y., Luscombe, S., Steeves, T., & Sandor, P. (2012). Canadian Guidelines for the Evidence-Based Treatment of Tic Disorders: Pharmacotherapy. The Canadian Journal of Psychiatry, 57(3), 133–143. https://doi.org/10.1177/070674371205700302