From pubescence to menopause, people with ovaries and a uterus will likely menstruate. Menstruation changes the level of sex hormones in the body, which not only control and regulate the reproductive system, but also affect thinking, moods, behaviour, appetite and libido. The “Female Reproductive System” is often not taught well in general schooling and for those who were taught, they may have forgotten much of the detail, with the result that most people don’t know how their own bodies work and the effect this has on them.
What many people do not understand is how the reproductive cycle affects hormone levels, which directly affects how your brain neurology functions. There are two key points in the cycle where this can be felt, the Mid Cycle Crash and PMS, which in severe cases leads to PMDD (Pre-Menstrual Dysphoric Disorder).
You may also be interested in
- ADHD, PMDD, Mid Cycle Crash
- Postnatal Depression
- Neurology
- Nutrition and Diet
- Sleep
- Understanding Transgender
- Mental Health
- ADHD / Anxiety / Autism / OCD
- Narcissism
TL:DR Hormones, Brains and Menstruation
Hormone effects on cognition, mood and task energy:
- Primary Sex Hormones
- Oestrogen (estrogen for USA) and Progesterone, which have a direct effect on how much Oestradiol (estradiol) is available.
- Oestradiol and the Brain
- Oestradiol has a direct effect on the Dopaminergic System – the more Oestradiol, the more Dopaminergic Neurotransmitters
- Dopaminergic means Dopamine, Noradrenaline and Adrenaline, so low Oestradiol is a complicating factor for ADHD
- Dopamine = Cognition (thinking, solving, remembering, understanding)
- Noradrenaline = Mood regulation, Task Prioritisation and Impulsiveness Suppression
- Adrenaline = Task Completion Energy
- Oestradiol extra
- Oestradiol is one of the 4 possible forms of Oestrogen
- The other forms of Oestrogen, Progesterone and Testosterone will be broken down in your body, and one of those break down ingredients (for all the sex hormones) is Oestradiol
- In the USA they skip the O at the beginning of the Oestrogens, so they call it Estrogen and Estradiol.
Phases of the cycle:
- Follicular Phase: Reproductive system clears the uterus and matures an egg for ovulation.
- Menses is menstrual flow
- as
- A bit of pain and cramping is normal, strong pain is not.
- Often lasts around 5 days.
- Your body discharges blood during this time.
- Cognition (thinking) and mood can be low during this time, which can lead to some difficulties with behaviour. People can be feeling a level of fatigue due to low neuronal adrenaline.
- Middle of the Follicular Phase
- From the last day of menses to ovulation.
- Some people report that this is the best time of their month, where cognition and mood are best, and feeling energised.
- Ovulation
- Matured egg usually leaves the ovary. Sometimes it does not, which can exacerbate the Mid Cycle Crash.
- Menses is menstrual flow
- Luteal Phase: Reproductive System is creating an ideal environment for an embryo.
- Mid Cycle Crash
- Oestrogen and Progesterone become low, causing low Oestradiol, which causes low Dopamine, Noradrenaline and Adrenaline Neurotransmitters..
- Feeling like you have PMT for 1 to 2 days, about 3 days after you would have ovulated.
- Management: Be kind to yourself and if possible, delay hard tasks.
- Middle of the Luteal Phase
- Oestrogen and Progesterone are at their peak, often leading to Oestradiol peaking, which gives the best Dopamine, Noradrenaline and Adrenaline Neurotransmitter levels.
- Many people report this as the best time of their month, where thinking and feeling are working the best, and they feel energised to do things.
- PMT/PMS
- PMT (Pre-Menstrual Tension) PMS (Pre-Menstrual Stress)
- Hormones are at their lowest, disrupting the production of Dopamine, Noradrenaline and Adrenaline Neurotransmitters.
- Low A period of lowered Executive Function, higher emotions and reactivity.
- For people with low Oestradiol and or ADHD, this can often become PMDD (PreMenstrual Dysphoric Disorder), a period of odd behaviours, low cognition and heightened emotion
- Mid Cycle Crash
The rest of this gets pretty detailed and assumes little to no prior knowledge. Areas that I get very detailed in are behind a “In detail…” box.
Menstruation
The most common menstrual cycle is 28 days long. A variation between 25 to 30 days is considered to be within acceptable medical tolerance. If your menstrual cycle is outside of those on a regular basis, or frequently fluctuates significantly more than 4 or 5 days, then you should talk to your gynaecologist about this. If you don’t have a gynaecologist , talk to your GP and ask for one. While some GP’s are well educated and capable to handle odd reproductive issues, many are not – remember that GP stands for “General Practitioner” – they are not specialists.

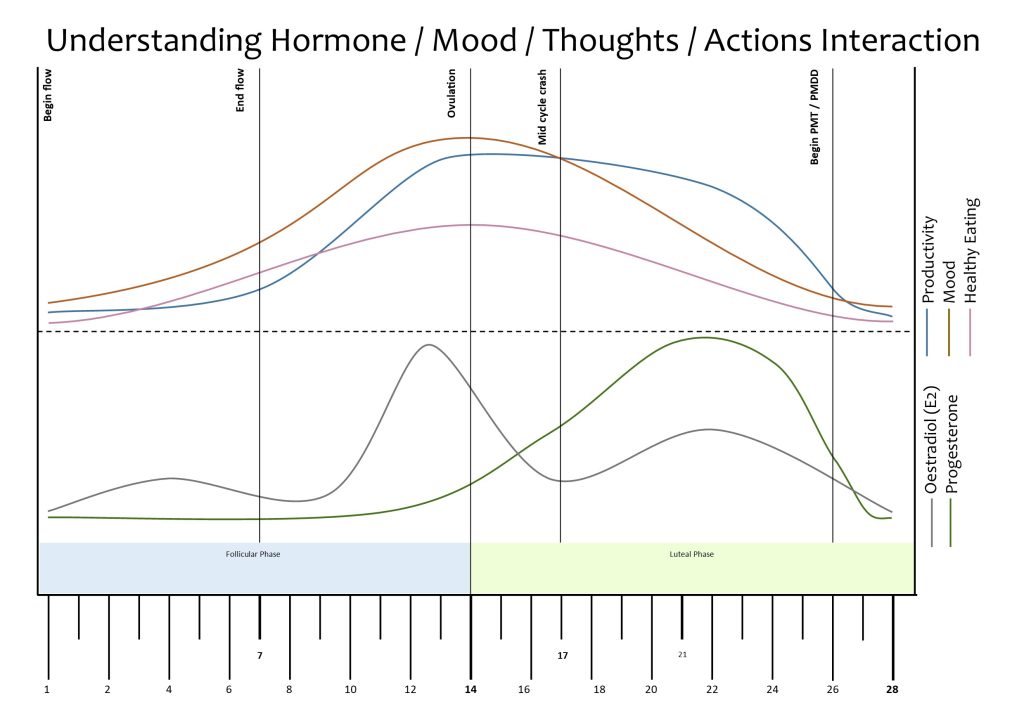
This is a graph of how the six major hormones appear across the menstrual cycle, separated into the Follicular Phase and the Luteal Phase. The vertical graph for each hormone is adjusted for clarity and to indicate the strength of the effect on the person. For example, Testosterone typically peaks at 0.171 mg/L while Progesterone typically peaks at 25 mg/L, which is too large a scale difference to see if we didn’t adjust each hormone to be clear.
Essentially, the Luteinising Hormone and Follicular Stimulating Hormone regulate which part of your period phase you are in. Generally, they are not too important, so here is another graph without them being included.

Follicular Phase
The Follicular Phase (FP), is considered to begin when menstruation begins, and concludes at Ovulation.
In detail… (click > for more)
FP is also known as the preovulatory phase or proliferative phase, is the phase of the menstrual cycle where follicles in the ovary mature from a primary follicle to a fully mature graafian follicle, developing an oocyte (proto egg) to maturity, ending in the release of that egg in Ovulation. You are born with your full complement of oocytes.
Follicular Stimulating Hormone and Luteinising Hormone, released by the pituitary gland in your brain, initially increases during menses, then decreases for around a week. It will sharply increase to its highest level as part of the process to trigger the egg to be released from the ovary, then rapidly decrease once the egg is released.
During the FP, a sack grows around the ovum that helps with fertility.
As the oocyte proto egg reaches maximum maturity, Oestrogen reaches its peak, which triggers the sharp rise of FSH and LH, which trigger the release of the egg.
Menses, AKA Menstrual Flow
Menstrual flow is the time of the cycle where you excrete the unused uterus lining. You will likely experience cramps and some minor pain. If you find that the cramps and pain are frequently so painful that they prevent you from doing things, you should get this assessed (details below). All of the hormones that regulate your menstrual flow are low, with FSH and LH rising.
At the start of the cycle, your primary sex hormones are near their lowest. Oestrogen and Progesterone have risen a little just after the low that triggers PMT and PMDD. Testosterone is on a slight rise, FSH (Follicle Stimulating Hormone) rises to around 2/3 of its peak monthly value white LH (Luteinizing Hormone) is dropping down. During this part of the cycle Oestrogen will begin to rise.
Typical Menstrual Flow
This commonly flows for between 4 to 6 days, however 2 to 8 days is considered within tolerance. The average is blood quantity over this time is around 30 mL of blood, about as much liquid as can be held in your hand that is slightly cupped with your fingers apart. The nominal range is from 0 mL to 80 mL (where 0 is no bleeding). In a more useful metric, if you need to change your tampon or pad more than every 2 hours, then you are likely bleeding heavily enough that you should talk to your doctor.
Menstrual clots (chunks) generally occur when the flow is heavy. They are more common during the first 2 days of menstruation, typically the heaviest part of a period.
Atypical Menstrual Flow
Greater than 80 mL and or flow that is greater than 8 days is considered concerning, and should be checked by your doctor. If this is occurring regularly and your doctor is not concerned, see the above section about “General Practitioner Doctors are not Specialists”.
For more information on this, consider this Heavy Periods link.
Managing Menstrual Flow
You can manage the excretions in a few ways, internal, external or combined. The most common four methods are tampons, menstrual cups, pads and menstrual pants.
Internal Flow Aids
Tampons are the most discreet but carry a bit of a higher infection risk than the other methods. This is mostly triggered by poor insertion methods and or not changing the tampon by the recommended manufacturer time. You can swim with tampons.
Menstrual Cups are an inserted device that look much like a flexible cup. This captures in the cup area the excretions of your period. You can then take the cup out, empty it, sterilise it and use it again. Cups can be initially tricky to insert correctly or remove without a mess, but this skill can be learned fairly easily. Much like reusable menstrual pants, menstrual cups are reusable, once rinsed and sterilised as per the manufacturer instructions. Much like tampons, most people find cups excellent, however some people find them very uncomfortable. Much like tampons, you can swim with a cup.
External Flow Aids
Pads line the underpants and absorb the discharge. Different sizes of pads have different amounts of absorption before they are full, so if your have a heavier flow you’ll benefit from a bigger pad. If the pad misaligns, there is a risk of bleeding around the pad and blood escaping your management system, which can be embarrassing if you don’t figure this out in time and if you don’t have some spare clothes. Pads are not compatible with swimming.
Reusable menstrual pants are now quite easy to purchase and address a great deal of the pad related problems. Reusable menstrual pants are basically underpants with build in reusable pads, but because they are designed for this, it is rare that there is spillage. As the name implies, these menstrual pants are reusable. To do so, thoroughly rinse them in cold water (either manually in a bucket, or a rinse cycle in your washing machine), then wash as a regular item with your clothes. It is a good idea to own several pairs, and remember to change them at least twice a day, when they feel soggy, or when they feel full. While regular reusable menstrual pants are not a good idea to swim in (as they leak and chlorine can damage them), you can get specific swimwear that works similarly and is suitable for swimming.
For more information on these, check out A quick guide to the Menstrual Cycle 2023 PDF and Period Education.
Managing Menstrual Pain
During menstruation the muscles around your uterus will contract to help dislodge the uterine lining. This can cause some discomfort and occasional pain. The pain can be felt in the middle front of your torso, between your belly button and your pelvic bone or where most people have the top part of their pubic hair.
The nerve that helps you feel your uterus is shared by the muscles on either side of the spine at your lower back, leading to referred pain, where your uterus is uncomfortable and your brain mistakes the pain as being from your back. Your brain’s response to this referred pain is to shore up the spine by stiffening the muscles, which then fatigue and ache. You can relieve this by using heat, stretches and various pain relief medication (eg naproxen and ibuprofen). Additional areas you may be feeling frequent co-occurring referred pain is your upper inner thighs and your hips.
You should not be feeling intense pain, dizziness or nausea. If you find that you become non-functional because of these symptoms (such as wanting to stay in bed curled up in a pain ball, or that you find it hard to focus because of pain), then you should talk to your GP about seeing a gynaecologist for Dysmenorrhea (painful menstrual cramps). While this level of pain isn’t necessarily an indication that something is broken or medically concerning, it both may be that something is concerning and should be addressed, or there are more medical grade treatments available to decrease that pain if there is no health concern. These treatments are often a more specific range of pain medications (eg buscopan, celecoxib and Panadol Osteo).
Menstruation and Toileting
Many people will find that their faeces changes consistency during this period of time. If your stool becomes hard, pellet like or you are constipated, you can try eating fruit, dried fruit or taking a medical stool softener to keep your bowel flowing properly. If you find that your stool becomes soft and runny, perhaps even diarrhoea, then you may need to take some medical aid to help firm that back up. A good consistent stool is an important marker for a healthy gut system, and we need those nutrients.
Transmen
Some transmen have periods. Not all male toilets have specialised bins for menstrual waste, facilities to get emergency supplies or safe access to a sink. In some regions, it can be dangerous to ask a fellow male toilet user for assistance, whereas it is generally safe to ask fellow women for support.
Depending on your region, if you can avoid a men’s bathroom and use a disabled / family bathroom, that is better. Generally, they have better default facilities, such as easy to access sinks, sanitary waste bins etc.
Plan ahead and be prepared. Basically, have a menstruation kit so you can have necessary supplies and ziplock (bags to put used items and dispose of them later [not the menstrual pants!]).
If you aren’t expecting your period, have a default pad or similar that you carry in your standard backpack, satchel or equipment. Admittedly, it is hard to carry useful supplies in just a wallet.
When you are expecting your period, carry a supply of pads, tampons, etc and a waterproof pouch, like a ziplock bag, that you can put used goods into. While not ideal, if there is no sanitary waste bin, you can dispose of these items safely later. Menstrual pants can make it a great deal easier to manage, are generally considered to be comfortable and you don’t need to change anything for around 12 hours, generally more than enough time to get to a safe place to change. Many trans masc folks report that some hygiene methods give them less dysphoria than others, and which ones varies from person to person.
We discuss other aspects of Transgender here.
End of Menses
Once your Menstrual Flow has finished, you should find that cramps and aches recede and your faeces return to normal. Generally, the cramps and aches recede prior to the end of flow, however a late cramp or some spotting (just a few drops of blood, not a flow) at the end is not too uncommon.
Ovulation
Ovulation is where the egg is released by the ovary approximately 14 days after the menstrual period. The range for ovulation is generally between 10 and 18 days, depending on the length of your regular period (if it is regular). The maximum fertility is a few days either side of ovulation as sperm can survive for a few days within the environment.
In detail…
The sharp rise in both FSH and LH are due to a feedback cycle from the increase of Oestrogen for the 12 to 24 hours at the end of the FP above. This surge lasts between 24 and 36 hours culminating in the now mature egg erupting from the follicle that was matured during FP above.
The released egg is caught by the fimbriae at the end of the fallopian tube (hair-like protein appendages). There is a gap between the oviduct and the fallopian tube and sometimes eggs don’t make it to the uterus. The end of the fallopian tube is open, and sperm can make it past there and find the egg, potentially fertilising it where it can no longer get to the uterus, leading to an ectopic implantation of the ovary outside of the uterus. The mechanism that is supposed to guide the egg to the fallopian tube, and then down to the uterus is a carpet of cilia, little tendrils that undulate direct the egg in the correct direction, much like the cilia in your gut direct matter from your stomach towards your bowel. [“Cilia take the egg on a magic carpet ride”external LINK].
It is not well understood why the rise in testosterone occurs during ovulation. Current speculation is that it is related to which follicles and oocytes are matured. [“The Normal Menstrual Cycle and the Control of Ovulation” external LINK]. It rises around 26% at its peak just prior to ovulation.
Middle of the Follicular Phase
Some people report that the week after menses and up to ovulation is when they feel the best: cognitively, emotionally and energy wise. Take a look below at Middle of the Luteal Phase for some discussion on this.
Luteal Phase
The Luteal Phase (LP) covers the part of the beginning of menses (menstrual flow) to Ovulation. In this time period a proto egg in the ovary is being developed into a functional egg on the end of a follicle. The proto egg is called an oocyte. You were born with all of the oocytes.
After releasing the egg, the follicle in the ovary folds in on itself becoming a corpus luteum, a cluster of cells that produces the sex hormones oestrogen and progesterone. The hormones induce the endometrial glands to begin producing the proliferative endometrium and later the secretory endometrium. This is where the fertilised egg, the embryo, can implant and grow.
We are not going to cover pregnancy in this article. It is important to know that the reproductive system cycle is focused on reproduction of the species, thus in humans the monthly cycle to prepare for fertilisation. Upon failure to fertilise, the Follicular Phase is triggered, which starts with menses.
LP has two mini phases that can affect mood and thinking, the Mid Cycle Crash and PMT, which in severe cases is PMDD (PreMenstrual Dysphoric Disorder – a period of odd behaviours, low cognition and heightened emotion). Both of these are characterised by a strong decrease in Oestrogen and Progesterone. The mechanism for the mood changes appears to be Dopaminergic, that is related to how Oestradiol affects Dopamine, Noradrenaline and Adrenaline.
A significant part of creating (synthesising) neuronal Dopamine, from which neuronal Noradrenaline and Adrenaline are subsequently made, is based on Oestradiol modulating the amount of neuronal Dopamine that is synthesised. This appears to be a direct correlation. That is, more Oestradiol in your body, the more your brain synthesises Dopamine.
Dopamine, Noradrenaline and Adrenaline are vital neurotransmitters.
- Dopamine runs your Executive Function (understanding the situation, solving problems, retaining information)
- Noradrenaline runs your mood by determining your level of current safety (safe = joy, content, relaxation / not safe = fear, anger and disgust), and thus what you should prioritise as the next task (task initiation)
- Adrenaline fuels the actions of tasks being done, whether that is cognitive of physical, and runs your emergency response system (Freeze, Fawn, Flight and Fight)
Oestrogen, Progesterone and Testosterone all break down into Oestradiol. During both the Mid Cycle Crash and PMT/PMDD, the availability of all three of these hormones is low, which leads to low Oestradiol, which leads to low Dopamine synthesis, which leads to decreased Executive Function, impaired Mood and difficulties with tasks.
- Acute Stimulatory Effect of Estradiol on Striatal Dopamine Synthesis, 1995
- ADHD, PMDD, Mid Cycle Crash and Hormone Interactions
- Dopaminergic System
PMT/PMDD and the Mid Cycle Crash are covered in more detail below.
Mid Cycle Crash
The Mid Cycle Crash is generally felt around 3 days after ovulation should have occurred. Research on the Mid Cycle Crash is sparse. Most people experience a drop in mood insignificant enough to shrug off and ignore, but some find that they experience 24 to 48 hours of marked decrease in mood, heightened mood reactivity and a decrease in cognition.
As you can see on the graph, this is a time of low hormones, often not as low as PMT (covered below), but in sharp contrast to the level before and after this point. If you did not ovulate, your follicle doesn’t become a temporary boosting endocrine system, which leads to a lower level of hormones, and thus mood and cognitive function.
While this does not affect most people, enough of my clients have noted a mood and functionality drop at this time of month that I have found it helpful to explain that this day or two of struggle is part of a natural hormone fluctuation and not due to some past trauma or personal incompetence. The clients who this affects have reported back to me that when they feel unexpectedly bad, they check their menstrual tracker, note that it is the Mid Cycle Crash, and are more easily able to shrug off the secondary self blame effects that they usually have. They switch mode for the remainder of the day to “being kind to myself” and pick things up the next day (or the day after that if they have the 48 hour version).
Knowing why you feel how you do helps the negative self talk be less bad.
We cover this in more detail in ADHD, PMDD, Mid Cycle Crash and Hormone Interactions.
Middle of the Luteal Phase
After Ovulation and a possible Mid Cycle Crash, and prior to PMT, Oestrogen and Progesterone are at their natural peak. Assuming a successful ovulation, the temporary endocrine site from the Corpus Luteum adds a bit of extra Oestrogen and Progesterone to the system. Oestradiol is at the highest natural level of the month and that means that Dopamine, Noradrenaline and Adrenaline are at optimal values, leading to quick thinking (cognition), stable mood and energy to act on wants.
Many people report this as the best days of their menstrual cycle.
There are some people who find that they feel best just prior to ovulation. This may indicate that high Progesterone is limiting the production of Dopamine. So long as you do not feel cognitively or emotionally compromised, this is not a thing that needs to be medically addressed.
There are some who can become manic in this phase, which can be mistaken for Bipolar Affective Disorder. This is addressed in more detail in ADHD, PMDD, Mid Cycle Crash and Hormone Interactions.
PMT and PMDD
PMT (Pre Menstrual Tension) or PMS (Pre Menstrual Stress), is a difficult time just prior to menstrual flow. As you can see from the graph, all of the hormones are at their lowest. If you recall from above, Oestradiol directly affects the amount of Dopaminergic Neurotransmitters you have, effecting your cognition, mood and behaviour, and this time is month has the lowest Oestradiol level. During this phase, it is harder to think, mood is dysregulated, appetite is altered (often Dopamine chasing – aka junk food, or food avoidant), stool (faeces) often hardens but sometimes becomes loose (period poops), libido drops and decision making is poor.
For some, especially if you have ADHD, you can experience a severe effect to your cognition, mood and behaviour, leading to problematic behaviours as you lose or struggle to have conscious control of your choices. To make good choices, you need sufficient Dopamine in your Prefrontal Cortex and the right level of Noradrenaline in your Amygdala. Without those, your understanding is poor and your mood can’t be trusted. This is called Premenstrual Dysphoric Disorder (PMDD), which is covered in detail on our PMDD page.