This topic is mostly taboo for no good reason, ignorance is not a protective factor. Most people do not casually consider the option to take their own lives, or harm themself, let alone act on it. Suicidal Ideation is the serious thought about killing yourself, while Suicide or Suicide Attempt is the action taken to kill yourself, even if you survive it. Self Harm Ideation or Thoughts of Self Harm are similar to the use of Ideation above, but for self harm. Self Harm or Deliberate Self Harm are the terms used when the harm is actioned, even if the harm does not happen. Most of the driver for these are biological, usually neurotransmitter based or cardiopulmonary. The next most common driver is social, then economic and the least likely is a cognitive error / psychological.
You may also like
- Crisis
- Anxiety
- Other Mental Health
- Neurology
- Nutrition and Diet
- Sleep
Taboo, or not Taboo
As stated in the introduction, talking about Suicide and Self Harm is mostly taboo.
People shy away from talking about killing yourself and harming yourself, often citing the reason as their fear that openly discussing this will enable you to kill or harm yourself as feasible options. They fear that by having a discussion about when this might be okay, or what it means when someone feels like this is going to increase the number of deaths or permanent injuries.
There is no better evidence for this than for schools who teach the history of World War 2 causing more wars. If anything, proper education about war leads to a reduction of war, and there is good evidence that teaching about Suicide and Self Harm lead to a reduction in Suicide and Self Harm (Ref 1, Ref 2). Considering that, perhaps we should review making this topic a taboo?
The more we don’t talk about it, the more that people who are experiencing this feel alone,
making it harder for them to reach out for help,
and the less other people know about this and what to do when someone does reach out for help.
Definitions
Click to expand (Defining terms around Suicide and Self Harm)
- Suicidal Ideation
- The serious thought about killing yourself as an option or drive.
- This can include researching how to kill yourself or fantasising about killing youself.
- Researching how to die may be a curiosity, sense of completeness act, and should not be included as ideation if there is no interest in using this knowledge (that is, the thought of acting on this research wasn’t the driver of the research).
- Suicide / Suicide Attempt
- The act of killing yourself, even if you survive it.
- Self Harm Ideation / Thoughts of Self Harm
- Similar to the ideation for suicide, where hurting yourself seems to be a realistic option.
- This can look like researching how to harm yourself, or fantasising about hurting yourself.
- Researching how to harm yourself may be a curiosity, sense of completeness act, and should not be included as ideation if there is no interest in using this knowledge (that is, the thought of acting on this research wasn’t the driver of the research).
- Self Harm / Deliberate Self Harm
- The act of physically hurting yourself.
- This can look like cutting your skin, bruising yourself, concussing yourself, or any other form of injury that will take a day or more to heal.
- Medically, the term “self harm” or “deliberate self harm” glosses over:
- Social self harm
- Financial self harm
- Dietary self harm
- Slow physical self harm (such as smoking, alcohol misuse or medication refusal).
- The word “deliberate” is often used to make it clear that this doesn’t include an accident, it is intentional. Personally, I think this is unnecesarry.
- The act of physically hurting yourself.
Understanding Self Harm and Suicide
People who were born feeling like they should take their life generally did not pass their genes on. That is, this is not a natural state for us to frequently find ourselves in. There are some hypothetical situations where taking hurting yourself and or taking your own life is the right choice. For this to be true, though, the situation must be extreme.
While evolutionary psychology has some evidence based flaws (that is, it is hard to prove the hypothesis is right or wrong), it can give us some useful conceptual models for understanding ourselves. As George Box points out, “essentially, all models are wrong, bust some are useful”.
Reasonable Choice to Self Harm
Aron Ralston is famous for getting pinned by a dislodged boulder while solo climbing in Utah. After five days, he recognised the the chances of him randomly being rescued were too low and his best option was to break his forearm and amputate his forearm so that he could get to where people were likely to find him. While it is possible that he might have got rescued if he waited longer, his chances of survival were far less likely than if he self harmed and left the canyon. [Ref 8].
Aron’s situation is one of those extreme circumstances where harming yourself makes sense. A far more common circumstances is when we agree to a medical operation. Every operation does some harm, but that is balanced by the recognition that the procedure will most likely result in greater good than doing nothing. When you sign the consent form, you are deliberately agreeing to be hurt, even though it is for someone else to do the harm to you. Everyone who has elected to get a tattoo has also agreed to be hurt, however in this case, in comparison to a medical operation, there is no greater harm you are avoiding by this form of self harm.
Reasonable Choice to Die
Liviu Librescu, a holocaust survivor, was a teacher at Virginia Tech in 2007 when the school was accosted by a lone shooter. Librescu closed the door to the classroom and used his own body to barricade it to stop the assailant. While he was shot four times by the gunman, the students managed to kick open a window and escape. Librescu died as a result of his actions. One student, Panchal, was lying next to Librescu, also shot and wounded, when the gunman forced his way into the room. He shot them both in the temple, killing them. [Ref 9].
Librescu was in an extreme circumstance, where he elected to likely die to save many others. This wasn’t the first time that Librescu had faced death, being a survivor of the Jewish Holocaust. Librescu made a deliberate decision to act as a shield to his students, recognising that he would likely die. Even if he thought he might somehow bluff the attacker to not come in the room, after the first shot through the door, Librescu must have known that his chance of death in pursuing his decision to act as a shield was very high, yet he persisted in blocking the door.
1st July 2021, Western Australia allowed Voluntary Assisted Dying (VAD), aka euthanasia, reflecting the new Voluntary Assisted Dying Act 2019 [Ref 10]. This enables adults who have decision making capacity to apply for and potentially receive VAD if they have a suitable diagnosis of a disease, illness or medical condition, that is advanced, progress and will cause death within 6-12 months (depending) with no reasonable medical treatment that allows for the time until death to be tolerable. For example, painful stage 4 cancer where no medication adequately relieves the pain. If granted, the person will have an assisted death before their ‘natural’ time if not assisted.
The reason for discussing these situations is to point out that humans have the built in mechanisms that in some instances allows them to decide that harming themself or taking their own life is a valid option, and that people do make these choices, often without negative judgement.
Unreasonable Choice to ‘Self Harm’ or ‘Die’
When we generally refer to someone who is self harming or suicidal, we mean something different to the above “reasonable” times. We mean someone who is choosing to harm themself or take their life in a situation that does not look necessary or wise- it seems irrational. The mechanism for self harm or killing themself has been triggered, but the known circumstances does not seem to be a valid cause.
So what is going on here?
I have worked with many people who have problems with self harm and suicide. Whenever a person I have worked with or interviewed after the fact has felt that they needed to act on the thoughts regarding self harm or suicide, they were not in a stable mental state. They were acting as if they were in a critical situation where their survival brain was making decisions. Let me explain.
Simplifying a lot, we have 3 main Brain Modes, aka 3 types of thinking.
- Cognitive
- Brain Mode 1: Question & Answer Sets
- Fast, efficient
- Inflexible
- Brain Mode 2: Novel Problem Solving
- Slow, costly
- Super flexible
- Brain Mode 1: Question & Answer Sets
- Reflex
- Brain Mode 3: Survival Brain
- Fast, efficient
- Cunning
- Often harmful if there isn’t a specific crisis
- Brain Mode 3: Survival Brain
Brain Mode 1: Question & Answer Sets
The most common that you see is the Brain Mode that matches known answers to understand questions. This is a Cognitive Mode that works on defaults.
Eg 1: What is 2 + 2 ?
Eg 2: What is your capital city?
Most people reading the first example would have read the question and rapidly had the answer supplied to them by their brain without having to do any calculations or finding enough objects to play this through. Most people reading the second example would either know the capital, or not. Thinking more on the second example isn’t going to get you the answer if you don’t actually know.
You either know the answer, or you don’t. On your own, you won’t solve it if you don’t know.
This kind of Brain Mode finds answers so known complex problems quickly and efficiently. It is fairly fast and fairly cheap.
Brain Mode 2: Novel Problem Solving
The second type of Brain Mode we have is the the mode where we solve unknown questions. That is, I ask you question that you don’t have a matching answer already known, so you have to figure out what the question means, and then what the best answer might be, or go and do some work to find out more information to solve that problem. This is a cognitive mode that works on logic and reason.
EG: the capital city of the UK is London, the capital city of France is Paris. Is London bigger than Paris?
To answer this question, first we need to grapple with, what is meant by “bigger”?
Viable answers might be:
- Static population,
- total population (including tourists),
- building size,
- square metres,
- profit,
- assets…
Once you’ve decoded what bigger means, you then have to find out the information for both cities before you can answer that, which often means figuring out where to get that information from, going to look for it and then solving the initial problem.
The main point here is, when you are solving an unknown, you are cognitively calculating and consciously thinking it through. This thinking is slow and expensive, but powerful.
Brain Mode 3: Survival Brain
The last kind of Brain Mode is our Survival Brain, which we prioritise when we go into Survival Mode.
Ideally, when we are faced with a big enough threat, we will switch off our slow cognitive thinking and check to see if we have a “Brain Mode 1 : Question and Answer Set”, that is, do we already know what to do?
In the absence of a known answer, we switch to the default Survival Brain Solutions: Freeze, Fawn, Flight or Fight – pick one.
Our Survival Brain is all about getting through this problem we perceive before us, preferably alive.
Alive doesn’t mean happy, or intact. Our survival brain is cunning, not smart.
Sometimes our more Cognitive Brain recognises that our Survival Brain is making a bad decision and may challenge the plan. Our Survival Brain will often come up with a convincing lie that any rational person would scoff at, but due to the impairment to our cognitive function, our Barin Mode 2 will just accept this cunning rationale as truth, even though it is probably wrong.
“Sure, some people might miss me when I’m dead, but since I’m such a burden, they’ll soon realise they are better off.”
– common reasoning from a suicidal person (Red Flag Thinking).
When we recover from being in survival mode, we often retain these illogical answers and continue to believe them without properly using critical thinking.
“Hey, do you know someone who took their life? Yes? Did you ever get over their death? No? Then why would people get over yours?”
– prompt to check for sound reasoning (counterfactual)
A significant difference between the examples I gave that most people judge the person is making the right choice and the examples where someone is impaired, is that the first group mostly had extreme circumstances occurring around them and were making seemingly rational choices over time, while the people that we consider are making poor choices are not thinking rationally, and their circumstances to not justify the extreme action they are thinking.
That is, external circumstances didn’t drive them into survival brain, where in the right external circumstances sometimes we make the hard decisions. Instead, something has mistakenly led this person’s brain to go into survival mode that isn’t driven by external circumstances, leading to an ill informed rational for making a decision to harm themself or take their life that does not meet the situation. That is, to the external person, this makes no sense, but to the person taking action, it does. It is delusional, because the person’s brain lacks capacity to make rational decisions based on proper facts, that match the circumstance. Instead the person is making logical decisions, based on feeling led erroneous facts in a circumstance they are mis-perceiving.
People don’t enter Survival Mode randomly. Their is always a cause for it, even if we aren’t sure what that is. Generally, it is biological in nature, sometimes it is social pressure, rarely we have learned a thought pattern that is adversarial to ourselves. We will cover those in Primary Causes below.
Leaving Survival Mode Ideation
Many people experience transitory risk of self harm or suicide. Once the circumstance or biological glitch is addressed, the ideation for self harm and suicide disappears. That is, when the driver into Survival Mode is resolved, the cognition should return to the normal status quo, which should be no ideation for self harm or suicide, and no urge to risky acts. When there is no reason to consider death or self harm as a solution, you should leave these ideas behind.
However, there are many people who have frequent or constant ideation, even if they have no specific plan to act on the thoughts. Most of this cohort of people describe the thoughts as intrusive. They aren’t seeking these thoughts, the thoughts are entering their awareness uninvited. For some reason, the people in this cohort are stuck in some form of Survival Mode, so their thoughts are stuck on contemplating, or ideating, death and harm.
Let is separate an idle thought from ideation.
If I were to talk about oceans, your mind might just volunteer an idle thought about a related topic such as whales and sharks. That isn’t an intrusion of thought, that is an anticipation for what might be related and discussed. An intrusion would be where I talk about the ocean, and you think about how many bricks you can fit into your freezer. The extraneous thought is a non-sequitur, it doesn’t connect in a reasonable way to what I am saying about the ocean. Bricks aren’t considered distressing though, so we will generally dismiss that unconnected thought and try to focus back to the topic about oceans
Medically speaking, we would not count the unconnected thought about bricks in a freezer as intrusive as likely didn’t distress you.
Let us say it wasn’t “how many bricks you can fit in your freezer”, but perhaps “how many (insert things you’d expect to find in a horror film) into a freezer”, and that you find this distressing.
Medically speaking, we would now count that as intrusive thought rather than a random unconnected speculation.
Ideation outside of being in the Survival Mode is most often caused by adrenaline. To understand that, we need to first visit the concept of the Goldilocks Zone. There is an amount of adrenaline for our body and brain that is good and useful. However, if the level is too low, or too high, that can cause some major problems.
When our adrenaline (and noradrenaline) is low, our brain compensates by trying to do things to increase activity to prompt the release of adrenaline. We will feel like something is wrong and our brain will try to supply a reason to explain that. The reason will try to fit one of the 4 F categories:
- Freeze
- Fawn
- Flight
- Fight
The most common is by triggering aggression (fight) or anxiety (flight). Aggression is usually subconsciously looking for things to be angry at, so that you can justify a fight. Anxiety is usually subconsciously looking for things to be scared of, to explain the feeling that something is wrong.
When the adrenalines become critically low, we first start thinking about self harm, and if it gets worse, we think about suicide. This triggers a physiological emergency response, which releases emergency stores of adrenaline, and hopefully we can then stop the harmful behaviour.
Most death is caused by accident – that isn’t the actually outcome the person wanted.
“Imagine there are two magic doors before you. If you go through the first door, your life gets better. Whatever is causing you to think that death is a good idea has been resolved and no longer causes you problems. If you go through the second door, you die without mess. Which door do you choose?”
Most people who talk about dying, once they have had a bit of time to think about what the two doors mean, choose Door 1. They may struggle to tell you what is different in the life they now have, because it can be hard to know what is driving the ideation, or if known, clearly hard to address without help.
Very few people, upon consideration, actually choose Door 2.
If the adrenaline is too high, it can trigger a similar outcome, but the mechanism isn’t seeking adrenaline to compensate, it is now trying to explain the excess of adrenaline the brain finds. The part of the brain that prepares for disaster assumes that if adrenaline is present at high levels, then there must be a reason for it, and tries to find it.
The reasons our brain concocts to explain the need to raise adrenaline, or explain high adrenaline, seem super real and hard to spot as false.
That seems like an awful process. Evolution doesn’t have to work well, it just has to work. Different parts of our brain don’t get complex information from other parts, such as “hey, we need some more adrenaline, can you just make some more?” Instead, the brain part makes a local change that will trigger a distant part to respond, except there is no “why do this” transmitted. Imagine you are in a group of people and you need the person over the other side of the room to do something complex – but you can’t use any words (written, signed or spoken). Nor can you directly communicate with them, just with those near you. You might eventually get them to do what you need them to do, but the odds of them knowing why are low, leading to problems when you need them to change due to what you know, but they don’t. Truly, our brains could work so much more efficiently if the parts just talked better amongst themselves.
Pain can also cause this. Pain is not pleasant. To manage pain, we often use two neurotransmitters, endorphins and noradrenaline. The Endorphins that are used to manage pain are not available to be used for enjoyment, and the noradrenaline that is used to manage pain can lead to our brain doing the paragraphs above regarding adrenaline.
There are other medical conditions that can directly or indirectly throw our adrenaline system out of whack, leading to frequent and or persistent ideation.
Primary Causes
- Biological
- Socioeconomic
- Cognitive / Psychological
Biological
The vast majority of people who experience suicide and self harm are experiencing a biological problem. If you have been feeling suicidal ideation or thoughts of self harm for more than a few weeks, then the odds are moderate that you are experiencing a biological problem. If you have been feeling this intermittently or consistently for more than a few months, then the odds are very high that this is biological in nature.
Biological problems require biological solutions. You aren’t going to breath or meditate your way out of this.
In order, the most common are:
- Neurological / Neurotransmitter imbalance, mostly Noradrenaline, may be Dopamine, could be Endorphins / Oxytocin. This includes:
- Autism
- ADHD
- BPD / cPTSD / EUPD
- Bipolar
- PTSD
- Schizophrenia
- Psychosis
- etc
- Cardiopulmonary
- Heart or lungs
- Hormonal
- Very high or low estradiol
- Includes PMDD
- Thyroid
- Adrenal / Cortisol
- Very high or low estradiol
- Food Allergy / Intolerance, for example wheat, dairy.
- Most people do not experience ideation or action as a result of allergies and intolerances, but some do so it is important to consider if no other cause is apparent.
- Chronic condition, such as:
- Chronic Fatigue Syndrome
- Fibromyalgia
- Cancer
- etc
Most of these (1 to 4) can be addressed with medication, once diagnosed correctly. Unfortunately, chronic conditions can be very difficult to navigate, and may not respond well to medication.
A few words on Noradrenaline. Noradrenaline is the neurotransmitter that is used to manage our primary mood centre, the amygdala. It helps us determine if we are safe, and in the absence of that assurance, reports “not safe”. Most of the people who have seen me for suicidal and self harming concerns have had low Noradrenaline, and a NRI (eg Desvenlafaxine, Reboxetine or Edronax) have helped (when the person enjoys regular caffeine). However, around 10% have the opposite issue, where their Noradrenaline is mostly higher than the Goldilocks Zone (not too high, not too low), generally characterised by an avoidance of caffeine. For people in this category, Clonidine or a Beta Blocker is often helpful.
Neurodivergence, aka neurological differences, benefit from both medication, identity acceptance (see below for Identity), therapy for how to minimalise the friction of being neurodivergent, and social inclusion (also see Socioeconomic below).
Socioeconomic
A core part of our human identity is tied up our social identity and status. When we feel valued and welcomed, we want to live up to the idea and ideals of society. This is related to pedestalling (which can be misused), where when someone puts us on a pedestal of good behaviour (for positive versions), we want to do those good behaviours. When we are treated poorly by those we trust, given ambiguous cues about how we are doing in the group, and or treated like we are unwelcomed and useless, we will feel like we are a burden.
Not Belonging
There is a theorised biological driver for the people in a group (social) that are unneeded and draining the group to sacrifice themselves for the good of the group, likened to apoptosis (Ref 3) . In modern times, this “unneeded so sacrifice self” reality is a fiction, as we no long live in the environment that we evolved from, but the feeling can persist. We can always change groups, and no one who is kind is useless to a group (not that we should judge ‘worth’ on performance or what people provide). Unfortunately, when we think we have a good group and they do not value us (as defined by how they treat us, not their words), we can fall victim to this evolutionary biology drive to remove ourselves, mistaking that as we should die rather than remove ourselves from the group by finding a group that does value us.
Abuse / Toxic People
A single abusive person can cause us so much identity confusion that we can feel suicidal and try to kill ourselves. We may harm ourselves to try to mitigate death, hoping that this buys us enough time to find a solution. Sometimes we may struggle to identify that an abusive person is abusive.
Anecdotally, I have seen quite a few clients who were very distressed who completely failed to recognise that the primary source of their distress was their family member / spouse, because they were abusive. Upon the client distancing themselves from the person, they have generally decreased their distress, including ideation – especially when we have also worked to balance the rest of their brain health.
We have an extensive section for Abuse in our Conflict Pages.
Systemic Pressure
Organisations, like the government, can strongly influence people’s mental health. The way that employment agencies treat people while they are vulnerable can lead people to strong ideation. The Royal Commission into “Robo debt” recognised that at least 2030 of the almost 1 million people received a letter, died shortly afterwards. The letter from the government falsely and illegally claiming that the people had lied to the government about their income and now owed the government money.
It is not possible to prove how many of these suicides were wholly due to the attempted ‘debt collection’ (“No evidence to show Robodebt caused more than 2,000 deaths”, RMIT, Ref 4). It is fair that it is unlikely that every person who suicided after receiving this repugnant letter did so due to the letter, but it is also not fair to say that only 2 people suicided after the letter as a result, especially as it was identified that around 1/3 of the recipients were vulnerable people. “What is certain is that the Scheme was responsible for heartbreak and harm to family members of those who took their own lives because of the despair the Scheme caused them”, (Services Australia, Ref 5).
The government denies that all 2030 deaths were caused by their letter. The Royal Commission only directly reviewed a few of these deaths and concluded that these were fairly attributed to the robodebt, but did not acknowledge that the ones they did not review may have been. The assumption that the deaths were not caused by the letter seems to lean heavily on the investigation by the department who sent the letter concluding that it wasn’t responsible – the same department that knowingly broke the law to send the letter. The Royal Commission focused on the fact that Mr Tudge wanted to ensure that DHS’s (Department of Human Services) interactions with Mr Cauzzo “were appropriate and undertaken within the parameters of departmental processes.” The Royal Commission found that Mr Tudge’s “conclusions were wrong and the letter misleading. The error was not minor, and Mr Cauzzo’s case was not handled appropriately or sensitively.” Services Australia (Ref 5).
The Royal Commission also notes that despite the deaths that were being noted to DHS, “the Robodebt scheme doubtless caused significant harm, and can be blamed for multiple deaths including suicides — as the findings of the royal commission make clear — the figure is thought to be much lower than the number being cited online” (Ref 6). The Royal Commission found that “While each of those deaths may have prompted an internal review of the particular case, they did not galvanise either DHS or DSS into a substantive or systemic review of the problem of illegal, inaccurate or unfair debt-raising.” Services Australia (Ref 5).
I feel that the title from RMIT “no evidence to show Robodebt caused more than 2,00 deaths” is deliberately misleading – it caused at least 2, probably much more, but no one felt it important to confirm how many were directly, significantly contributed to by Robodebt.
Financial
Struggling finances is well recognised as a significant burden to people’s state of wellbeing, and can negatively affect people’s self worth, increasing risk of suicide and self harm. “Suicide is the 15th leading cause of death worldwide, with over 75% of suicides occurring in low-income and middle-income countries”, (Ref 7). The meta study just quoted found “a consistent trend at the individual level indicating that poverty, particularly in the form of worse economic status, diminished wealth, and unemployment is associated with suicidal ideations and behaviours” (Ref 7).
Cognitive / Psychological
Psychological distress is the least likely cause for long term suicide and self harm risk, but is the leading cause for short term risk. Psychological distress can come from a few different sources.
Most of the people who experience the drive to suicide or self harm are experiencing a biological problem, and often the cognitive / psychological reasoning they give is their internal post rationalisation for the biological driver.
Circumstance Driver
When we come across a problem, we try to solve it using the knowledge, skills and resources that we have available. Some of these problems will come with biological or socioeconomic factors, and may well be in the list above, such as ill health, job loss, financial hardship or organisation based bureaucratic adversity. If we can solve those factors, then we reduce that distress.
We first search our memory for this same problem, or if necessary, one like it, try to recall the solutions that we used for that and see if it will work in this situation. If it will, and we have the resources and skills necessary, we try it and see if it will work. If it does, no distress.
If it doesn’t, we become distressed. We will try various solutions, both hypothetically and practically, until either we solve the problem to a satisfactory degree, or we fail. Upon failure, we don’t know what to do.
For some people, this is very distressing, to the point of triggering consideration of self harm, or even suicide.
This is the time to seek help from other people, especially a social work therapist. While a psychologist can handle some of the problems you may face around this, the social work therapist has a set of skills in working within systems to find solutions, while most psychologists don’t.
Cognitive Driver
A Cognitive Driver is an idea that you think is true that leads you to conclude that something must be done for some reason, and that something is harming or killing yourself. An examples of this is a doomsday cult, where the person believes that the end is nigh, and thus the wisest thing to do is die first. While this might not look feasible to someone who has not had such thoughts, there is plenty of literature on people who have taken their own lives due to a faulty belief, such as doomsday cults.
The challenge of managing this driver is that the person at risk has frequently formed an illogical, nonsensical and irrational belief that leads to the conclusion that they should be hurt or die. It is very hard to use logic to undo illogic. Rational reasoning is for rational people.
Steps to help someone out of this are:
- Learn about their paradigm, that is their beliefs.
- Check for biological drivers, such as background anxiety disorders, neurodivergence and body health problems, and try to get those addressed.
- Attempt to use mainstream logic and facts to show that their reasoning behind self harm and death are illogical.
- In the high likelihood that this fails, attempt to use their paradigm to show the contradictions that undermine their internal rationale for the risky behaviour.
Identity Driver
While we are all human, there is a great deal of diversity in who we are within humanity. You may identify yourself as a type of person that differentiates you from others in a particular way that other people do not assume is true, or that your biology may not connect to. For example, you may view yourself as kind while the people in your social group claim that you are selfish (such as abusive situations, where they claim selfishness when you try to assert reasonable boundaries), or you may identify as a gender that does not match your biological sex markers, or you may be AuDHD and people are trying to treat you as a neurotypical person.
When your inner identity is at odds to how people treat you, this creates a pressure that leads to a heightened risk of suicide and self harm. For example, the risk of suicide in gender dysmorphia is around 20%. One person affirming the right of the individual to identify as they feel they are, affirming their gender identity over biological markers, can significantly reduce that risk of suicide.
What To Do
Since Self harm and suicide are quite complex, there is no single simple thing one should do. Depending on the circumstances will depend on the course of action. If a person has a good Safety Plan, follow it (the definition of a “good safety plan” is below in Safety Plans).
In the absence of a safety plan, then this is generally what you should do…
Helping Someone in Crisis
- During the Crisis: – high risk
- A person that is planning to act, or taking action is in Crisis, they will be in Survival Brain Mode.
- Generally, people don’t stay in Survival Mode for long.
- To check:
- Cognitive Test: ask them a complex question that they can normally answer. If you don’t know them, ask a two part question that most people could answer
- Eg: I have a meeting on Monday that I can’t make. I should move it forwards a day. I also struggle to think quickly before I have my lunch. What day and time should I ask them to make it?
- If they can’t, then their cognition is compromised.
- Behaviours: their actions will be odd (atypical) compared to what you know about them.
- Sometimes that will be agitated walking or movements, sometimes it will be pacing, sometimes it will be repeating the same phrase or movement.
- Cognitive Test: ask them a complex question that they can normally answer. If you don’t know them, ask a two part question that most people could answer
- While they are in Survival Brain Mode, they are in Crisis and their decisions are compromised.
- They are at high risk of acting with bad consequences.
- They are not “rational” in the mainstream sense (they think they are).
- What to do:
- Ask if they have a Safety Plan. If they can access it for you (or you can safely get it), follow it.
- If not,:
- Food:
- If they are not allergic or intolerant, prompt them to eat some food and have a cup of tea.
- Meds:
- Check that they took their medication. If they didn’t, give it to them.
- If they did, ask what PRN (as needed) medication they have for this (if it is a common event).
- Useful medications: benzodiazepine family (valium etc), antipsychotic, beta blocker, clonidine
- Avoid: alcohol, cannabis, opioids unless prescribed
- Distract them:
- How:
- Movies / TV
- Read to them / tell them an engagint story
- Talk about their special interest, try to engage them in it.
- Sometimes useful, make mistakes about their special interest. So long as they read this as a chance to correct you, rather than getting angry about your mistakes, it is working. If they get angry, that may fuel them to regrettable actions.
- How long:
- While the food and meds kick in, usually about 30 to 60 minutes.
- If they didn’t eat or take medication, then this could take 4 or more hours.
- It’s generally over when they fall asleep (meds), or are being Brain Mode 2 Rational.
- How:
- Food:
- They may need confinement (psych ward) if you can’t distract them from acting on risky behaviour.
- A person that is planning to act, or taking action is in Crisis, they will be in Survival Brain Mode.
- After the Crisis:
- Connect to a good therapist, doctor and posisbly psychiatrist.
- Determine the source
- As in, what caused the Survival Mode (mostly often biological, rarely circumstances)
- Track the pattern
- Times of Risk
- Differentiating between ideation, plan to act and taking action
- Frequency (how often)
- Severity (how strong is the urge)
- Duration (how long does the urge sit at that level)
- What preceded the time of Risk
- What and when was the last meal
- What and when was the last medication
- What is the sleep for the last 24 hours, compare that to the last 3 days
- If you have a menstrual cycle, where are you in that?
- What was your mood for the prior 6 hours?
- Not what the average mood was.
- Note any unusual large fluctuations in that.
- Times of Risk
- Have a Safety Plan:
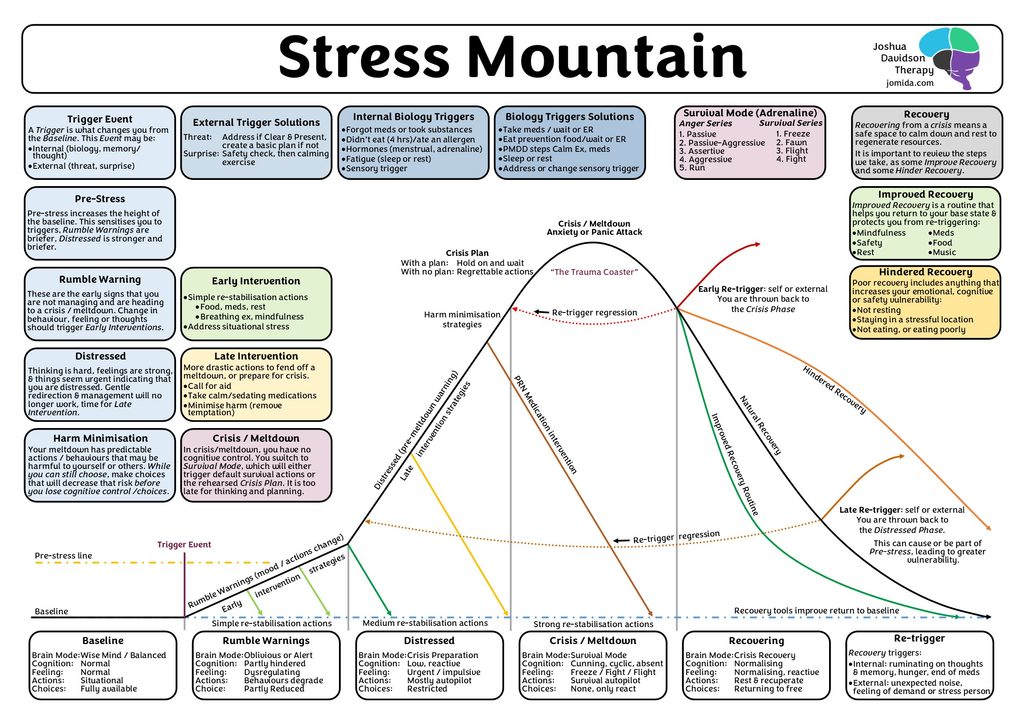
- Stress Mountain
- Safety and Wellness Plan
- 6 Most Common Causes (of weird behaviour, odd thoughts and strange moods)
This is a general flow chart to indicate what to do for a range of people. Not all of this is suitable for every person.
If the person has a good safety plan, follow it, since that is their wishes. Note the critiques of Safety Plans in the section Safety Plans if you have time.
Understanding the Cognition Question
The example question to test the person’s cognitive function is this:
“I have a meeting on Monday that I can’t make. I should move it forwards a day.
I also struggle to think quickly before I have my lunch.
What day and time should I ask them to make it?”
This question asks the person to solve a problem that requires them to cognitive engage with the elements of the problem to understand it, then to work a solution that will address the problem.
Part 1: If I say I have a meeting on Wednesday that I can’t meet, and I need to move it forwards 1 day, 50% of people will think you mean Monday, and the other 50% of people will think you mean Friday because “move it forward” is ambiguous due to the subjective way that people conceive of calendar time. In this case, because the original meeting is on Monday, the people who want to move it to the day prior, need to recognise that most meetings, implying business, don’t happen on Sunday, so therefore when you ask “what day”, it must mean Tuesday.
Part 2: I want the person to solve a second problem, the time of day. If I were to say “I don’t want to meet in the morning”, then they can use Brain Mode 1: opposite of morning is afternoon, which isn’t cerebral enough to be a good test. By pointing out a problem with thinking well prior to lunch, the person has to work out that this means “morning” and equate it to “morning bad”. The prompt of “what time” should result in “afternoon”.
This is broken down so that you can understand why this is a good two part question that most people should be able to answer, or at least, explain their reasoning to demonstrate why their answer is rational. That pushes a person to use Problem Understanding AND Problem Solving, which is Brain Mode 2.
Safety Plans
A good Safety Plan follows the changing capability of the person a la Stress Mountain. That means that intervention strategies like “breathing exercise” or “meditation” are in the Rumble Phase, as these only work as Early Interventions and fail as Late Interventions. Usually, by the time someone needs to intercede, the person is now in the Distress Phase. The Distress Phase requires Late Intervention strategies: removing self or stressor, seek help, medication, harm minimisation.
Many of the safety plans I have read for people completely fail to include any form of understanding about how cognition and emotional ability decline / decompensate as someone shifts to Survival Brain. Often these “safety plans” seem to work on the model of “just make different choices” on a background assumption that the person at risk has their full cognitive and emotional faculties. That just doesn’t work. Then again, that is mostly because people don’t understand what drives suicidality and self harm.
Ideal Safety Plan
- A good safety plan is a dynamic document.
- That is, it evolves over time. As you discover things that don’t work well for you, change them. As you discover things that work well for you, add them in. As your “safe contact list” changes, update it.
- Understand the phases of Stress Mountain.
- The purpose of this is to understand how Cognition, Emotion and Choice can change as you go up to a Crisis and enter Survival Mode, and thus why the Early Intervention and Late Intervention strategies need to be quite different.
- Base line – everything is good, you have lots of choices.
- Goal: maintain good mental health and functioning. That is, eat good food, exercise daily (if medically safe), take your medications, get good sleep, maintain good social.
- Rumble Warning – recognise the early signs that something is off.
- If the spoons you have or think you have no longer match the thing you are doing or planning to do, you will get Rumble Warnings.
- You choices will be somewhat reduced and your mood will likely be a bit out.
- Interoception: looking within to assess your internal state.
- This can be physical behavioural changes, mood change, cognition change, fatigue, feeling like you are being forced into something
- Identify the thing that is wrong and address it.
- Meds, Food, Hormones, Fatigue, Sensory
- This is all part of 6 Most Common Causes (of weird behaviour, odd thoughts and strange moods)
- Early intervention strategies:
- Breathing exercise
- Meditation
- Affirmation / Mantras / Prayer
- If this works, you should return to your baseline
- be gentle with yourself
- Distress Phase – a sharp elevation in not coping signals.
- You have missed the easy path / timing to get back to your baseline.
- You will find that thinking is hard, you will feel an urgent need to act in some way that is likely not actually good for you. Choices are now limited to things you have practiced (when you weren’t compromised) or Freeze, Fawn, Flight, Fight.
- Late Intervention Strategies:
- 1. Removing yourself from the situation.
- Go to somewhere calmer and safe.
- If you are at risk, don’t go alone if you can help it.
- If someone won’t go with you, call someone on your phone.
- 2. Call for aid if you haven’t already done so.
- 3. Take PRN medication prescribed for you for this situation.
- If this works, you will return to base line. Be gentle with yourself for a few to 24 hours to avoid retriggering.
- 1. Removing yourself from the situation.
- Harm minimisation:
- Move away from the common methods of harm that you are prone to.
- Seek help:
- Someone you trust in person or call a friend.
- If you can’t get a friend, call the MH or Suicide help lines.
- Go to psych ward if you can’t contain yourself from taking our life. Call an ambulance if needed, ignore the cost.
- Crisis Phase.
- Hold on and wait.
- You have little to no cognitive decision making here. You may think you are making smart choices, but you probably aren’t. Your emotions are likely lying to you, which is strongly interfering with your ability to make wise decisions. You have almost no choices and it is hard to resist taking action based on those faulty thoughts.
- Mantra: “Nothing can go wrong if I just sit down and wait.”
- Recovery Phase.
- We will return to baseline at some point.
- Improve recovery: you may have some things you do that speed this up.
- Impeded recovery: you may do some things that you think are good, but actually aren’t.
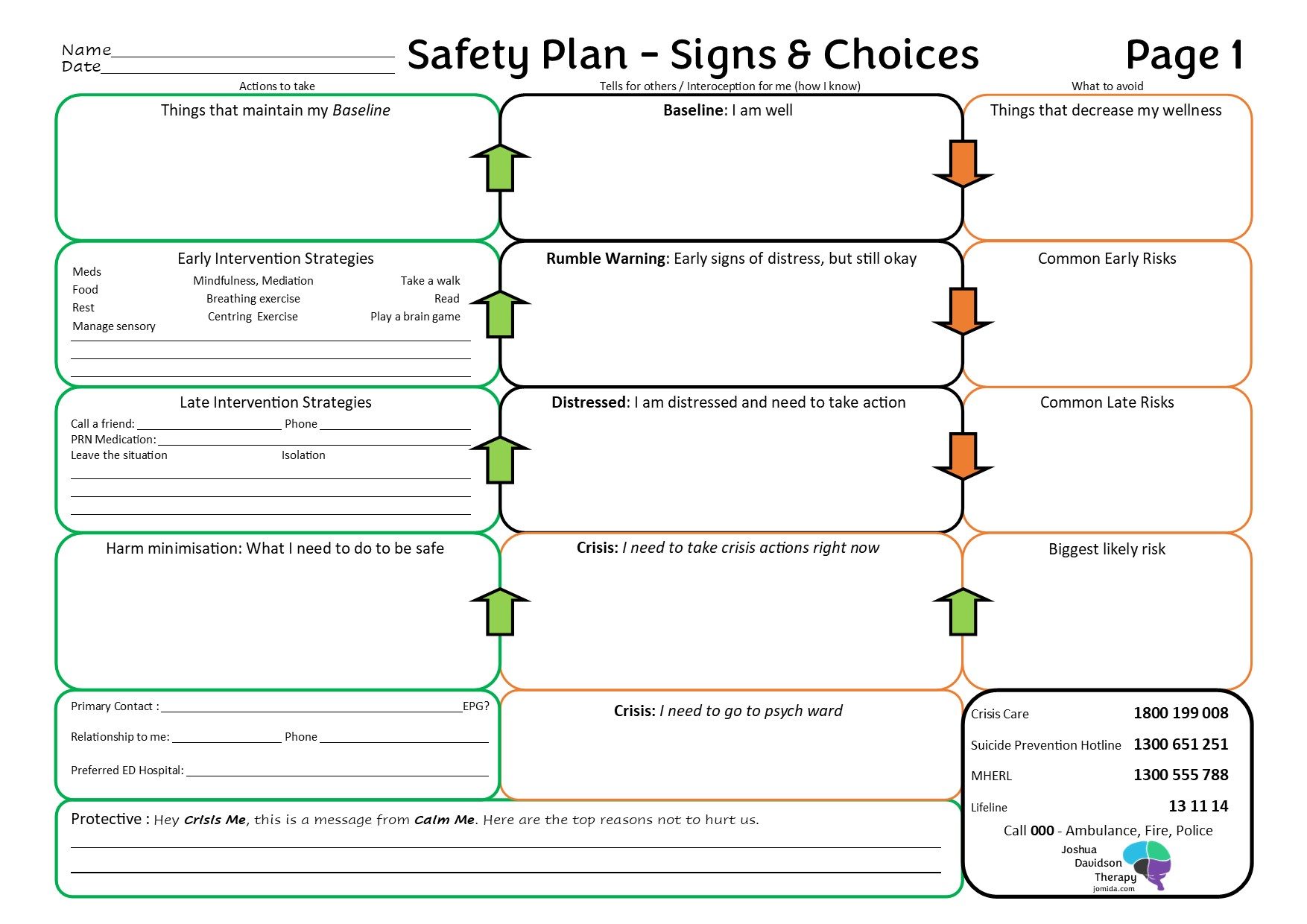
- Look at the Safety and Wellness Plan. Fill it in.
- Side 1
- The purpose of this form is to help you identify what you look like at Base, Rumble and Distressed, and what you should do for these steps.
- Assessing you
- 1. Fill in the middle box, top line, the “tells”, the thoughts and behaviours you do that indicate that you are in a good place (baseline).
- This encourages interoception, the ability to look within and know your inner state, or to observe your own behaviours and notice a change.
- 2. Fill in the left top box, the things that help you maintain your baseline.
- 3. Fill in the top right box, the things you know can compromise your baseline / wellbeing, such that you are now on the next line down, the Rumble Warning.
- Repeat the above 3 points for the second line, Rumble Warnings. Note that ‘2.’ is now “Early Intervention Strategies“.
- Repeat for Distressed. ‘2.’ is now “Late Intervention Strategies“.
- Crisis: I need to take Crisis Action
- Middle Box: List how you and how someone else would tell that you are in crisis.
- Harm Minimisation: List what do you need to do to be safe.
- Biggest Likely Risk: List what is the most likely thing you do would do that brings risk to yourself. This should be addressed in the Left box, Harm Minimisation.
- Crisis: I need to go to psych ward: List what it looks like when you can no longer keep yourself safe and you need to be contained at psych ward.
- 1. Fill in the middle box, top line, the “tells”, the thoughts and behaviours you do that indicate that you are in a good place (baseline).
- Primary Emergency Contact Person and Preferred ED Hospital.
- The last thing you want to be doing in a Crisis, when you are in Survival Brain Mode and can’t think properly, is trying to work out who you can trust and which hospital you would prefer to go to.
- Who do you trust to help you, who is accessible, and who can represent your best interests.
- Make sure you give them the latest version of this completed form, and a copy of Stress Mountain, and Top 6 Causes.
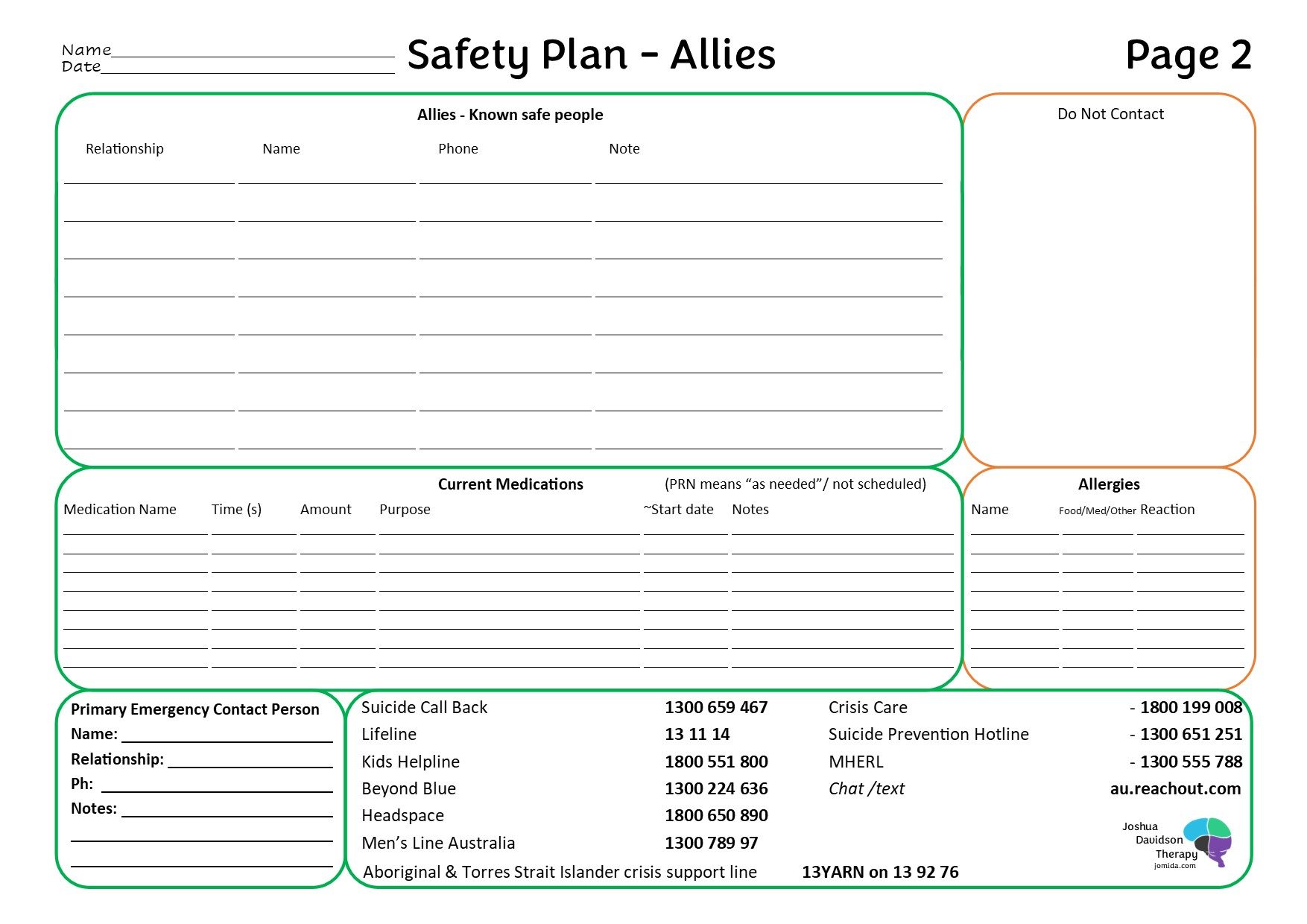
- Side 2
- When you are in Crisis, you are in Survival Brain Mode.
- That means it is hard to think and remember.
- Filling this in when you are calm and in control helps guide what happens when you are not calm and not able to think or choose wisely.
- Trust your calm self, who wrote this earlier.
- Allies
- Those who you can trust.
- “Note” information can include availability, or for what you find them good at doing for you when you are in crisis.
- Do Not Contact
- Most people have at least 1 person that is not good to be contacted. Often it is a family member, or an ex partner or an ex friend. Without specifying this, people might contact them by default.
- It is okay if you don’t have anyone to put in this box, of if you don’t feel safe putting someone in this box.
- Medications
- Update this whenever you change a medication.
- If you need to go to hospital, bring this with you.
- Allergies and Intolerances
- List what you are allergic to and what you are intollerant to.
- Not everyone knows what you are allergic or intolerant to, especially hospitals. Listing it here means you don’t have to have a clear mind to give them this information.
- When you are in Crisis, you are in Survival Brain Mode.
References
- Pistone, I., Beckman, U., Eriksson, E., Lagerlöf, H., & Sager, M. (2019). The effects of educational interventions on suicide: A systematic review and meta-analysis. International Journal of Social Psychiatry, 65(5), 399–412. https://doi.org/10.1177/0020764019852655
- Katalin Szanto, MD; Sandor Kalmar, MD; Herbert Hendin, MD; Zoltan Rihmer, MD, PhD, DSc; J. John Mann, MD; (2023). A Suicide Prevention Program in a Region With a Very High Suicide Rate, Jamanetwork.com. https://jamanetwork.com/journals/jamapsychiatry/fullarticle/482395
- The Royal Commission into the Robodebt Scheme. (2023, July 12). Report. Royal Commission into the Robodebt Scheme. https://robodebt.royalcommission.gov.au/publications/report
- No evidence to show Robodebt caused more than 2,000 deaths. (n.d.). Www.rmit.edu.au. https://www.rmit.edu.au/news/factlab-meta/robodebt-not-directly-responsible-for-more-than-2000-deaths
- https://www.abc.net.au/news/david-campbell/9943000, & https://www.abc.net.au/news/ellen-mccutchan/9943250. (2023, August 3). Did 2,030 people really die as a result of the Robodebt scheme? ABC News. https://www.abc.net.au/news/2023-08-04/fact-check-2030-robodebt-deaths/102684206
- Bloom, H. (2001). Global brain: The evolution of mass mind from the big bang to the 21st century. John Wiley & Sons. https://www.researchgate.net/publication/246326945_Global_Brain_The_Evolution_of_Mass_Mind_From_the_Big_Bang_to_the_21st_Century
- Iemmi, V., Bantjes, J., Coast, E., Channer, K., Leone, T., McDaid, D., Palfreyman, A., Stephens, B., & Lund, C. (2016). Suicide and poverty in low-income and middle-income countries: a systematic review. The Lancet Psychiatry, 3(8), 774–783. https://doi.org/10.1016/s2215-0366(16)30066-9
- Wikipedia Contributors. (2019, December 22). Aron Ralston. Wikipedia; Wikimedia Foundation. https://en.wikipedia.org/wiki/Aron_Ralston
- Wikipedia Contributors. (2026, February 24). Liviu Librescu. Wikipedia; Wikimedia Foundation.
- Western Australian Legislation – Voluntary Assisted Dying Act 2019. (n.d.). Www.legislation.wa.gov.au. https://www.legislation.wa.gov.au/legislation/statutes.nsf/law_a147242.html
-