Autism is a highly hereditary congenital neurological condition that can be disabling, inconvenient and or enriching. Medical texts such as the USA’s DSM and UN’s ICD have diagnostic criteria that focuses on differentiating people who are classically struggling with Autism and people who are not struggling with Autism. The advent of Neurodivergence Theory has led to the re-recognition that Autism is a neurological condition, but further that Autism is not automatically a neurological disorder – it is a different, not a disability. The concept of Autism is evolving to better fit the population who are both diagnosed with Autism and self-identify as Autistic. Various languages around that evolution of Autism and old out of date standards and theories about what Autism was remain in the zeitgeist of social beliefs that are out of date, wrong and misleading. Perhaps the representation that is best suited to show Autism in a snapshot is the Autism Wheel, while low/high functioning, less and more Autistic and Autism Levels are worse than misleading.
You may also like
Autism in a Nutshell
We have covered what Autism is and isn’t before. Autism has a medical definition that is somewhat at odds to what it means to have an Autistic Brain and thus Autism Identity. The diagnostic criteria in the DSM and ICD are focusing on how to tell if a person is Autistic and needs support, thus worthy of a medical diagnosis. While this may be logistically useful for governments (and in some cases insurers), it does not really match how Autistic people see themselves.
That is, while the criteria for diagnosis does match some of the experiences of Autistic people, these differentiation points are mostly useful for diagnosis and miss much of what it means to be Autistic.
Humans vary. We may all run on red blood, but importantly we have around 50 different types of blood clustered in to 8 different lettered blood types. I may not be compatible with your blood. Ask any surgeon and they’ll tell you that while most people’s hearts are in the right place, most people’s hearts look quite different and lots of adjustments need to be made whenever work is done on the inside of the body.
Brains are no different. We all have different brains. Similar to hearts, the basic configuration is approximately the same for most of us, but no two brains are identical. Similar to blood type, we can cluster brains around different neurotypes. The biggest single group is commonly called Neurotypical, and any cluster group that is different to that biggest group is an example of Neurodivergent – neurologically divergent from the most common (average) group. The third biggest neuro group is called Autism (the largest is ADHD).
The defining trait for Autism is difficulties around socialising and communicating with Neurotypical people. Both ICD and DSM require that one of the traits of difference includes a social struggle of some kind. Modern research has found that often Autistic people do not struggle to communicate with other Autistic people – ranging from not struggle at all to not as much. The diagnostic criteria does not specify this, which can make diagnosis more complicated when Autistic people talk about their friends and don’t specify or know that those friends are Autistic too, and not enough diagnosticians remember (or know) to check.
ICD requires at least one non-social trait to do with patterns, rigid thinking or sensory issues, while DSM requires two.
Misleading Ideas about Autism
Disability and Intellectual Disability – Low and High Functioning
Autism was a term originally coined by Swiss psychiatrist Eugen Bleuler in 1911. He was describing the inwards attention of certain Schizophrenic patients (he also coined Schizophrenia) “Autismus”, and anglicised to “Autism” – Aut/Auto meaning self, ism – to do / action aka inwards focus or in his words (translated to English) “morbid self-admiration”. Schizophrenia was a much broader diagnosis, which was used to describe any person that was odd. Childhood Schizophrenia was often the diagnosis given to children that we would now recognise as Autistic, not Schizophrenic. Leo Kanner‘s early work on what he called Infantile Autism began to separate the Autism as distinct from Schizophrenia, stating in 1943 that this group was recognised by their “powerful desire for aloneness” and “obsessive insistence on persistent sameness”. Kanner did go back and forth a bit in his view of this being distinct from Schizophrenia.
Historically, the majority of people diagnosed with the various versions of Autism were often Intellectually Disabled (historically, enfeebled, retardation and other older terms for this modern diagnosis). That is, there was a secondary condition, a comorbidity (existing in the same body) a diagnosable Intellectual Disability. Autism was often conflated with Intellectual Disability, with many assuming they were one and the same, or that the Autism aspect was secondary to the Intellectual Disability.
Once it was recognised that Autism was possible in people who were not Intellectually Disabled or disadvantaged, it became diagnostically relevant to separate the diagnosis of Autism from Intellectual Disability and clearly state if both diagnoses were present. Initially, Asperger’s Syndrome (Aspies) was the preferred descriptor for Autistic people without an Intellectual Disability.
Asperger’s Syndrome was named after the group of highly functional but odd people that met certain Autistic criteria but had no specific indication of Intellectual Disorder that Hans Asperger was investigating. This term has fallen out of favour due to complexities about nazi ideology. There is clear history that Hans Asperger worked hard to avoid nazi ideology and avoided nazi themes, however his work is viewed as nazi ideology and propaganda by others [1,2,3].
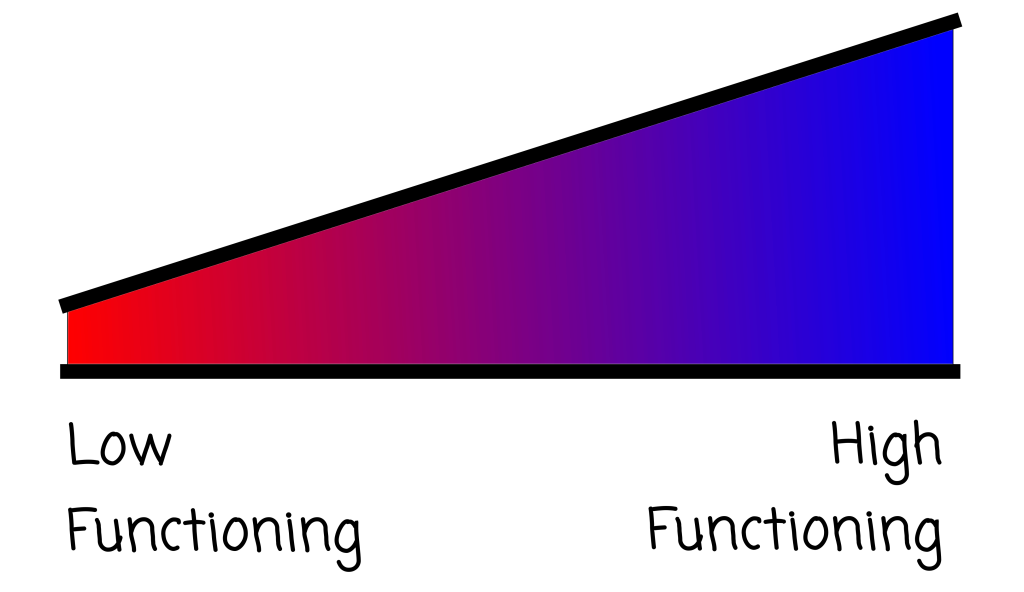
This led to the misleading description of Autistic people as either “low functioning” or “high functioning” [4,5], where low functioning referred to just Autism implying an Intellectual Disability and high functioning referred to Asperger’s Syndrome implying no Intellectual Disability. This misleads people as they are thinking about functional capacity when they reading “functioning”, not the absence or presence of a second comorbid diagnosis of Intellectual Disability.
More or Less Autistic
“Aren’t we all a bit Autistic?”
No. No we are not.
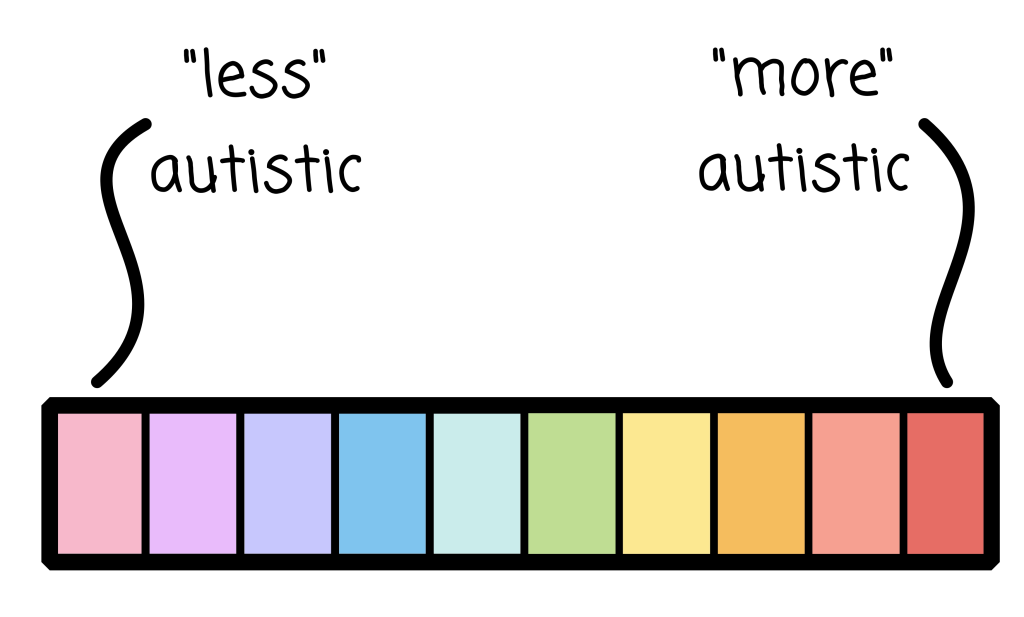
This is about as useful as saying “don’t we all experience menstruation?” Around half of the human population do not experience menstruation. Those who do will have a range of different experiences. It is tempting to suggest that people experience mild or severe menstruation, which is akin to the next type of common mistake about Autism, the “less” autistic or “more” autistic error. The medical diagnosis for Autism only outputs that a person is Autistic or is Not. We will cover the bit about “Levels” in the next section.
Let us look at menstruation for a moment. For those who are feeling a bit squeamish, perhaps try to recall that this is a frequent reality for half of the world’s humans for 20 to 30 years of their life. Some people have different levels of flow, cramping, pain, mood dysruption, cognitive dysruption and so on. What is tolerable for one person may not be well tolerated by another person. While someone could characterise this particular menstrual cycle as overall mild and perhaps the next one is severe, it would be unfair to assume that all future menstruations will be a reflection of this particular cycle.
Autism is similar, except there isn’t clearly defined cycles. Instead each Autistic trait you have will vary in personal experience based on factors such as fatigue, when you ate, how much sleep you’ve had, other stressors, level of sensory stimulation and so on. The trait that you are examining may benefit you, while for someone else, experiencing that same trait may be intolerable.
One of my clients finds that errors in documents leap out at them, which makes it profitable to be a copy editor, document analyist or code enterer. On the other hand, advertising and menus are painful. Does this trait make them more or less Autistic? Please point to where on this line this client should fit.
Sir Anthony Hopkins uses his hyperfocus and likely masking skill to be a world renowned actor. Hopkins states that he finds that social interactions and communication are tough for him, picking up social cue is difficult, certain noises and textures can be triggering to discomfort and he historically struggled to get employment. Hopkins has certainly struggled, but he’s also ritch and well respected. Does this make him mor or less Autistic? Please point to where on this line this client should fit.
Levels of Autism (Severity Specifiers) – 1, 2, 3
Bizarrely, the DSM 5, released in 2013, added an optional part to an Autism Diagnosis to write down the Severity Specifier Level of Autism.
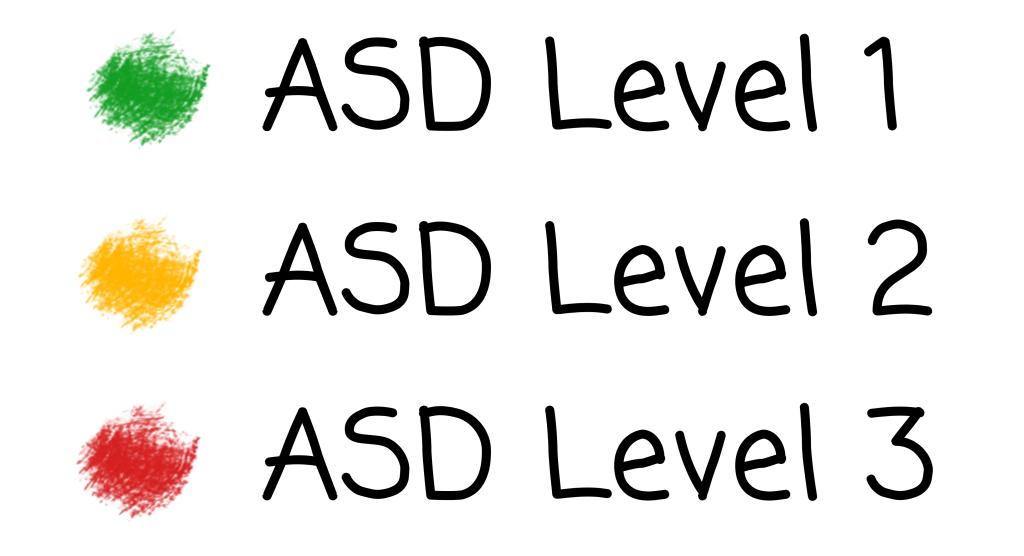
The DSM 5 define 3 levels of Severity Specifier [see Understanding Autism, the Medical Model for a full description and discussion]:
- Level 1 – Requiring support
- “Without supports in place, deficits in social communication cause noticeable impairments” etc
- Level 2 – Requiring substantial support
- “Marked deficits in verbal and nonverbal social communication skills” etc
- Level 3 – Requiring very substantial support
- “Severe deficits in verbal and nonverbal social communication skills cause severe impairments in functioning” etc
In Australia, the NDIS has latched on to this Severity Specifier to initially guide funding and supports. This has now evolved into a requirement which dictates funding for disability support for Autism.
What is concerning is that the DSM not only states that this is optional, but also:
“The severity specifiers (see Table 2) may be used to describe succinctly the current symptomatology (which might fall below level 1), with the recognition that severity may vary by context and fluctuate over time. Severity of social communication difficulties and restricted, repetitive behaviors should be separately rated. The descriptive severity categories should not be used to determine eligibility for and provision of services; these can only be developed at an individual level and through discussion of personal priorities and targets. Regarding the specifier “with or without accompanying intellectual impairment,” understanding the (often uneven) intellectual profile of a child or adult with autism spectrum disorder is necessary for interpreting diagnostic features. Separate estimates of verbal and nonverbal skills are necessary (e.g., using untimed nonverbal tests to assess potential strengths in individuals with limited language).”
Source for the above: Autism Aspergers Advocacy Australia, DSM 5 TR
I have boldened the very important sentences. To understand why this is useless, I have broken down the reasons here:
- “The severity specifiers (see Table 2) may be used to describe succinctly the current symptomatology (which might fall below level 1), with the recognition that severity may vary by context and fluctuate over time.”
- “may be used to describe” – optional to do this section
- “which might fall below level 1” – a person does not need to reach level 1 support to be diagnosed with Autism
- “with the recognition that severity may vary by context and fluctuate over time” – this Severity Specifier Level is only valid for the day it is measured as “severity may vary by context and fluctuate over time”
- “The descriptive severity categories should not be used to determine eligibility for and provision of services; these can only be developed at an individual level and through discussion of personal priorities and targets.”
- “The descriptive severity categories should not be used to determine eligibility for and provision of services” – which NDIS completly ignores
- “these can only be developed at an individual level and through discussion of personal priorities and targets” – because what is an impairment for one person may not be an impairment for another, and the number next to the Level (which is only valid on the day of assessment) does not define what specific support the individual needs.
TLDR: Level’s are only valid for the day of assessment, aren’t needed and shouldn’t be used to either restrict a person from a diagnosis or define what care support the person is elligble for or needs.
Autism Wheel / Flower – Best so far
Rebecca Burgess was frustrated with how people misrepresented Autism Spectrum, so for Autism Acceptance week back in 5 April 2016 on her tumblr page, she created a comic via her character Archie to explain how Autism is more like a colour wheel. This is the earliest I have found that Autism Spectrum has been displayed in a wheel with points from the distance showing the strength of a trait.
Dr Luke Beardon is the most common person credited with creating the Autism Wheel by AI, however I have emailed him and he denies having done so.
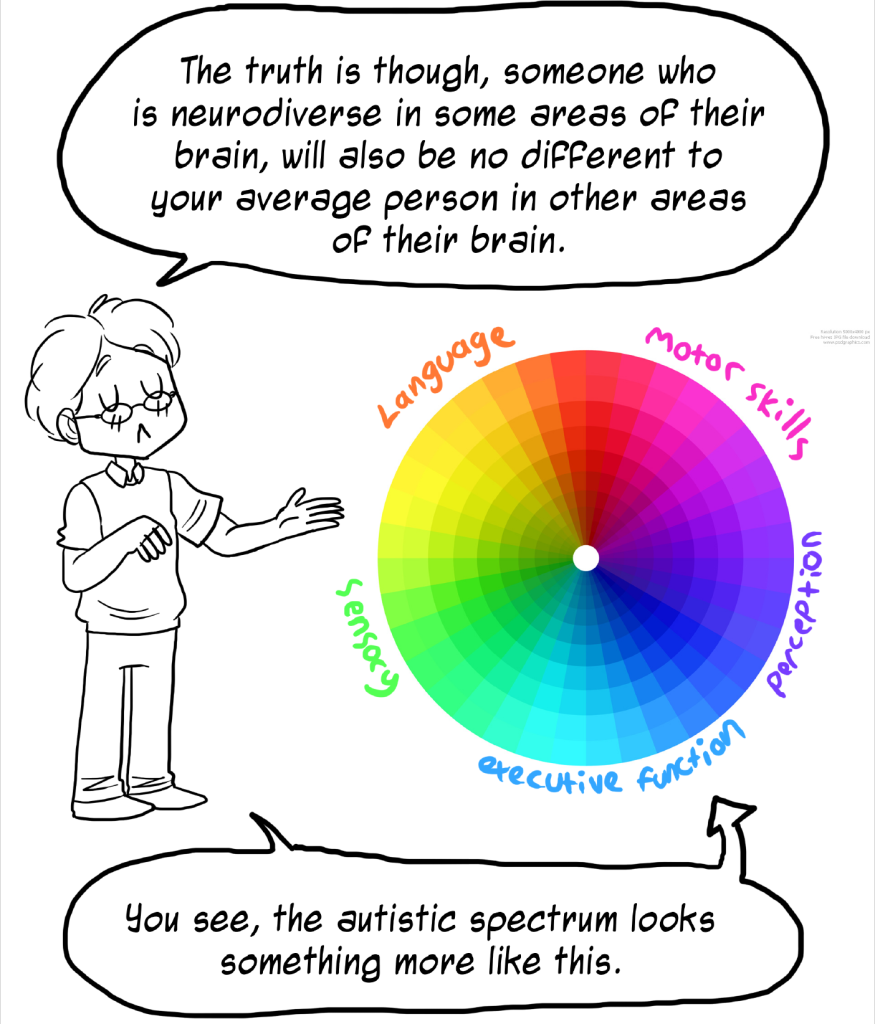
Images from “Understanding the Spectrum”, Rebecca Burgess, 5 April 2016 – showing the likely origin or inspiration of the Autism Wheel
The Autism Wheel shifts the paradigm of linear perception (as shown in the above 3 sections) of less to more Autistic to a pattern shown within a circle. Each slice of the wheel is a domain, representing the most common Autism trait tropes and a degree of difference from Neurotypical. These slices of the wheel are typically shown with 4 layers, 0 being neurotypical, 1 minor, 2 significant and 3 major deviation from the Neurotypical experience. A Neurotypical person would chart most of their answers within the inner markings towards the centre of the circle and an Autistic person would have at least 2 (ICD) / 3 (DSM) slices beyond the first marker.
There appears to be no standard number or naming for the domains, so the number of slices of the wheel can vary. There also appears to be no standard for how to create the Autism Wheel or how to interpret the Autism Wheel.
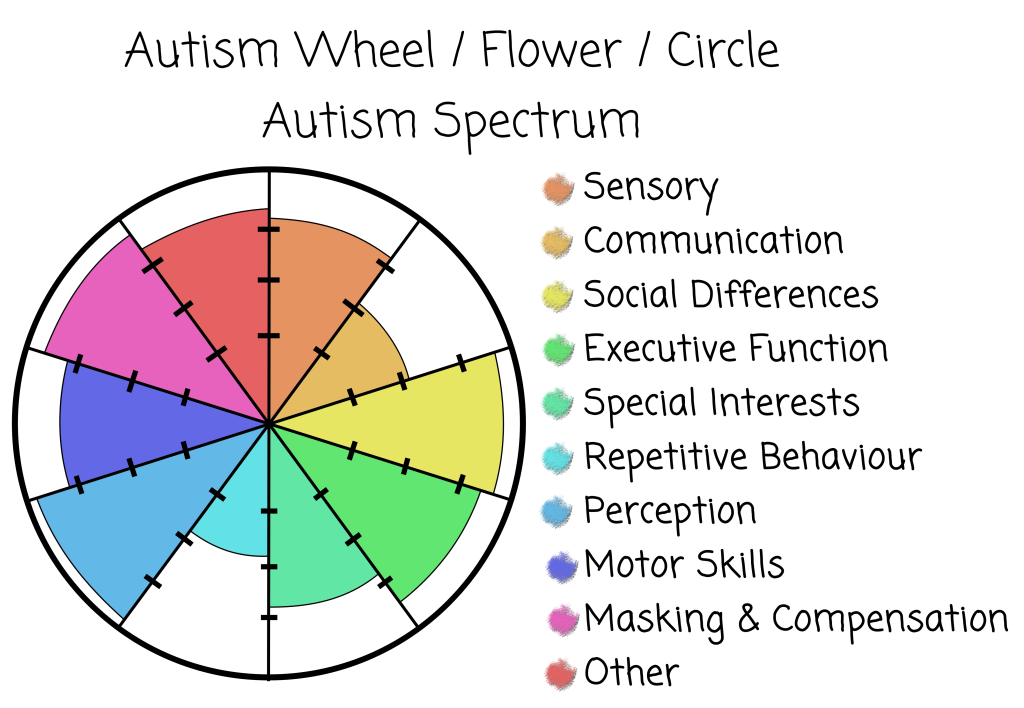
While this presentation shows a pictorial version of someone’s experience / traits, it doesn’t tell you why they have the amount of any slice, or if this particular domain represents a boon or burden. For example, you might have painful high sensory sensitivity to high pitch sounds (phobic high pitch hypersensitivity), but be excellent at managing loud sounds (hyposensitive to volume) while loving the sounds of bubble wrap popping (philic hypersensitive / ASMR). That’s just audio, which would be logged under the Sensory domain. This does not indicate how someone’s thermal sensitivity affects them (boon or burden), or textures, or … That is, a score of 3.2 in the Sensory domain shown in this graph doesn’t convey any important information beyond “perhaps you should ask”.
An advantage of the Autism Wheel over others is that it very much highlights the spectrum nature of Autism. Each person’s graph is going to be quite different to each other one, affirming that if you’ve met one Autistic person, you’ve met only one Autistic person (the other’s are different), and that an Autism presentation is noticeably different to the common central dot of neurotypical people. In this case, the Autism Wheel certainly meets Burgess’s intent and is by far the best way to quickly show someone how Autism is experienced differently for each person and why people refer to the Autism Spectrum.